

Cost Utility of Lifelong Immunoglobulin Replacement Therapy vs Hematopoietic Stem Cell Transplant to Treat Agammaglobulinemia
- PMID: 34779842
- PMCID: PMC8593831
- DOI: 10.1001/jamapediatrics.2021.4583
Cost Utility of Lifelong Immunoglobulin Replacement Therapy vs Hematopoietic Stem Cell Transplant to Treat Agammaglobulinemia
Abstract
Importance: Lifelong immunoglobulin replacement therapy (IRT) is standard-of-care treatment for congenital agammaglobulinemia but accrues high annual costs ($30 000-$90 000 per year) and decrements to quality of life over patients' life spans. Hematopoietic stem cell transplant (HSCT) offers an alternative 1-time therapy, but has high morbidity and mortality.
Objective: To evaluate the cost utility of IRT vs matched sibling donor (MSD) and matched unrelated donor (MUD) HSCT to treat patients with agammaglobulinemia in the US.
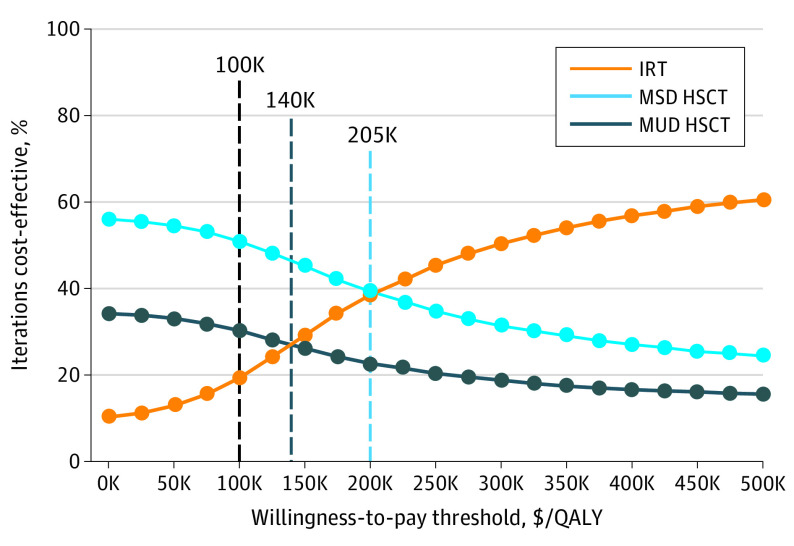
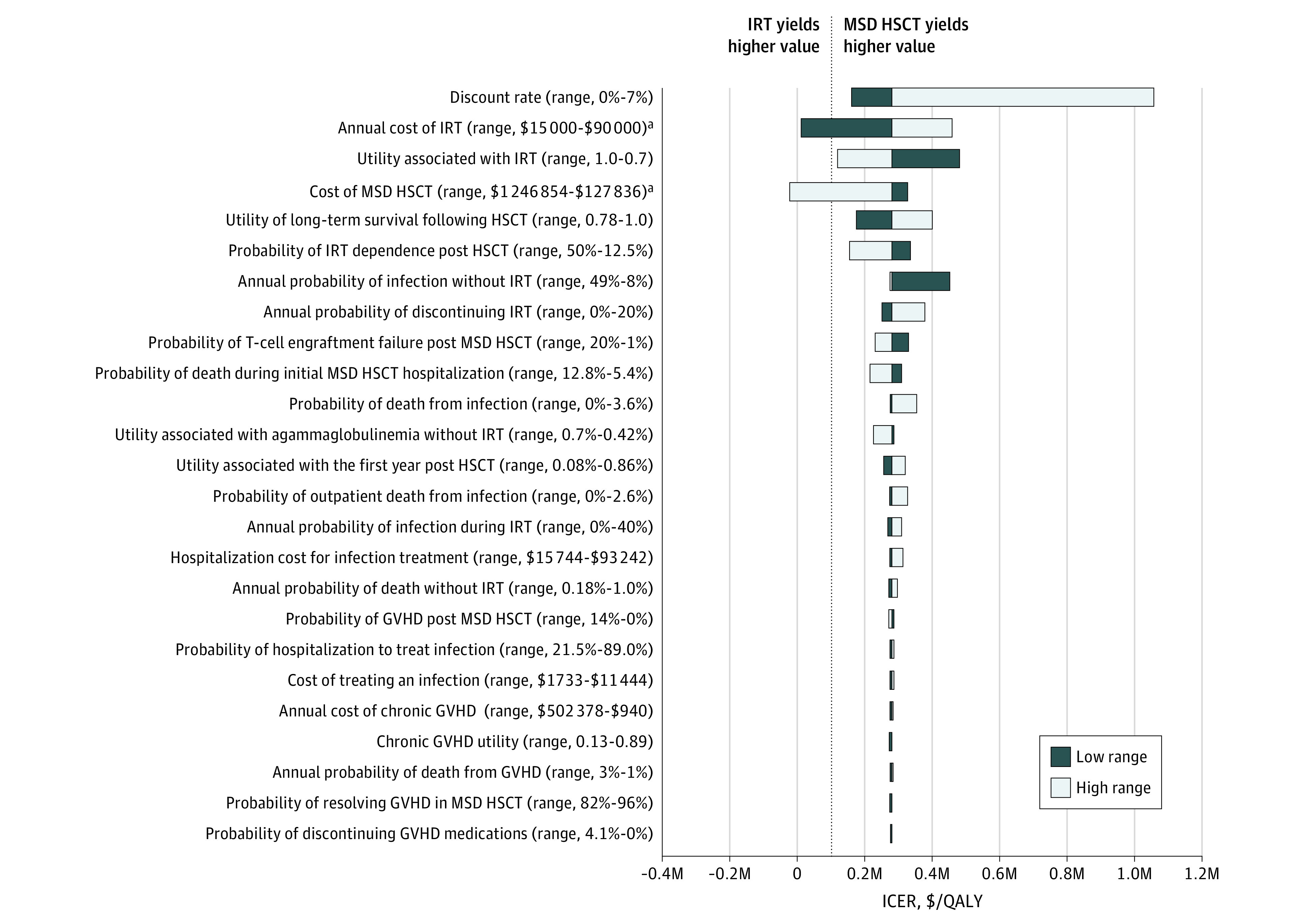
Design, setting, and participants: This economic evaluation used Markov analysis to model the base-case scenario of a patient aged 12 months with congenital agammaglobulinemia receiving lifelong IRT vs MSD or MUD HSCT. Costs, probabilities, and quality-of-life measures were derived from the literature. Microsimulations estimated premature deaths for each strategy in a virtual cohort. One-way sensitivity and probabilistic sensitivity analyses evaluated uncertainty around parameter estimates performed from a societal perspective over a 100-year time horizon. The threshold for cost-effective care was set at $100 000 per quality-adjusted life-year (QALY). This study was conducted from 2020 across a 100-year time horizon.
Exposures: Immunoglobulin replacement therapy vs MSD or MUD HSCT for treatment of congenital agammaglobulinemia.
Main outcomes and measures: The primary outcomes were incremental cost-effectiveness ratio (ICER) expressed in 2020 US dollars per QALY gained and premature deaths associated with each strategy.
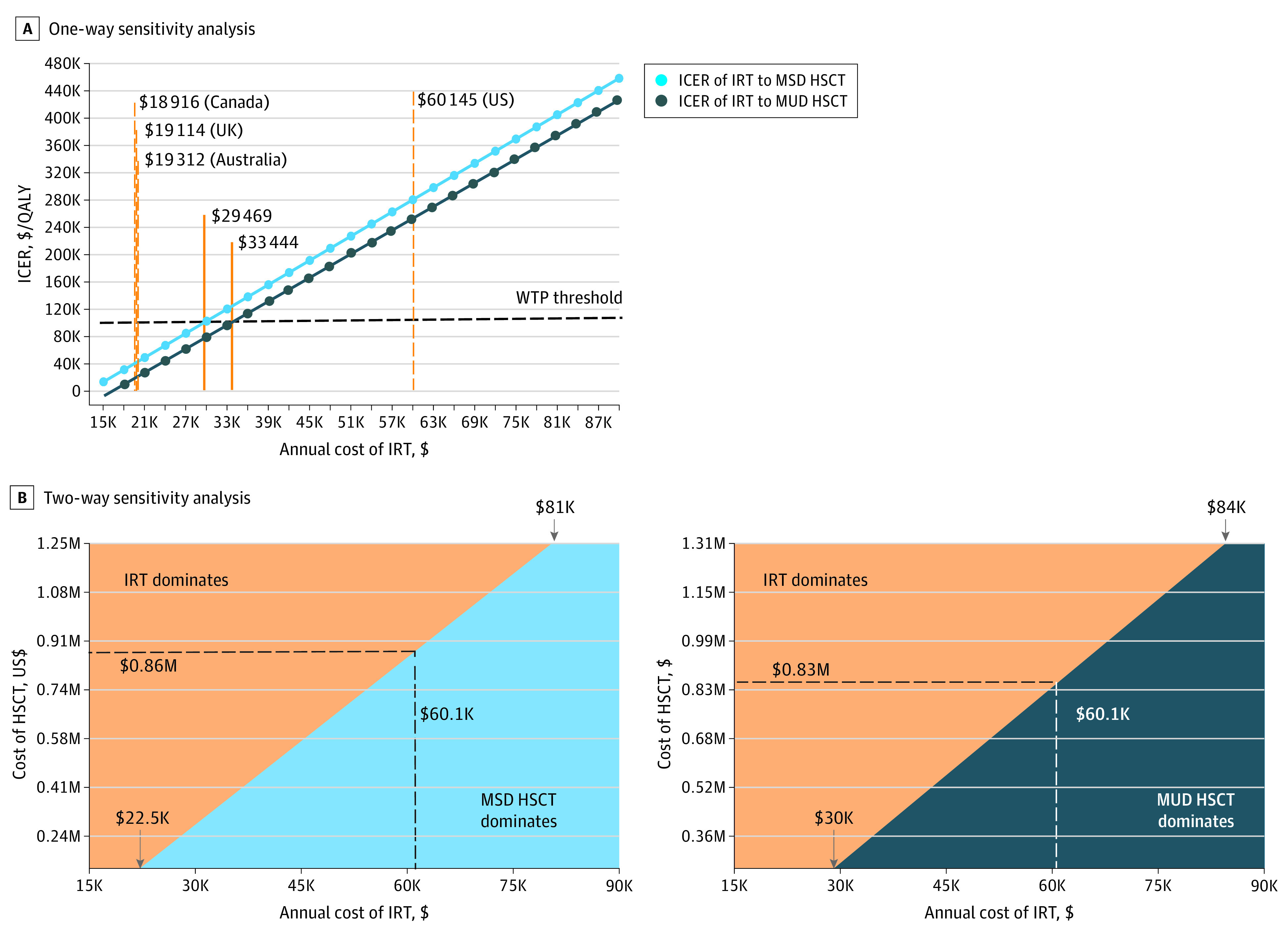
Results: In this economic evaluation of patients with congenital agammaglobulinemia, lifelong IRT cost more than HSCT ($1 512 946 compared with $563 776 [MSD] and $637 036 [MUD]) and generated similar QALYs (20.61 vs 17.25 [MSD] and 17.18 [MUD]). Choosing IRT over MSD or MUD HSCT yielded ICERs of $282 166 per QALY gained over MSD and $255 633 per QALY gained over MUD HSCT, exceeding the US willingness-to-pay threshold of $100 000/QALY. However, IRT prevented at least 2488 premature deaths per 10 000 microsimulations compared with HSCT. When annual IRT price was reduced from $60 145 to below $29 469, IRT became the cost-effective strategy. Findings remained robust in sensitivity and probabilistic sensitivity analyses.
Conclusions and relevance: In the US, IRT is more expensive than HSCT for agammaglobulinemia treatment. The findings of this study suggest that IRT prevents more premature deaths but does not substantially increase quality of life relative to HSCT. Reducing US IRT cost by 51% to a value similar to IRT prices in countries implementing value-based pricing may render it the more cost-effective strategy.
Conflict of interest statement
Figures
Comment in
-
High Drug Costs Hurt Health Outcomes-One Way or Another.JAMA Pediatr. 2022 Feb 1;176(2):131-132. doi: 10.1001/jamapediatrics.2021.4580. JAMA Pediatr. 2022. PMID: 34779826 No abstract available.
References
-
- Sullivan KE, Stiehm ER. Stiehm’s Immune Deficiencies Inborn Errors of Immunity. 2nd ed. Academic Press; 2020.
