

Assessment of Intercostal Nerve Block Analgesia for Thoracic Surgery: A Systematic Review and Meta-analysis
- PMID: 34779845
- PMCID: PMC8593761
- DOI: 10.1001/jamanetworkopen.2021.33394
Assessment of Intercostal Nerve Block Analgesia for Thoracic Surgery: A Systematic Review and Meta-analysis
Abstract
Importance: The use of intercostal nerve block (ICNB) analgesia with local anesthesia is common in thoracic surgery. However, the benefits and safety of ICNB among adult patients undergoing surgery is unknown.
Objective: To evaluate the analgesic benefits and safety of ICNB among adults undergoing thoracic surgery.
Data sources: A systematic search was performed in Ovid MEDLINE, Ovid Embase, Scopus, and the Cochrane Library databases using terms for ICNB and thoracic surgery (including thoracic surgery, thoracoscopy, thoracotomy, nerve block, intercostal nerves). The search and results were not limited by date, with the last search conducted on July 24, 2020.
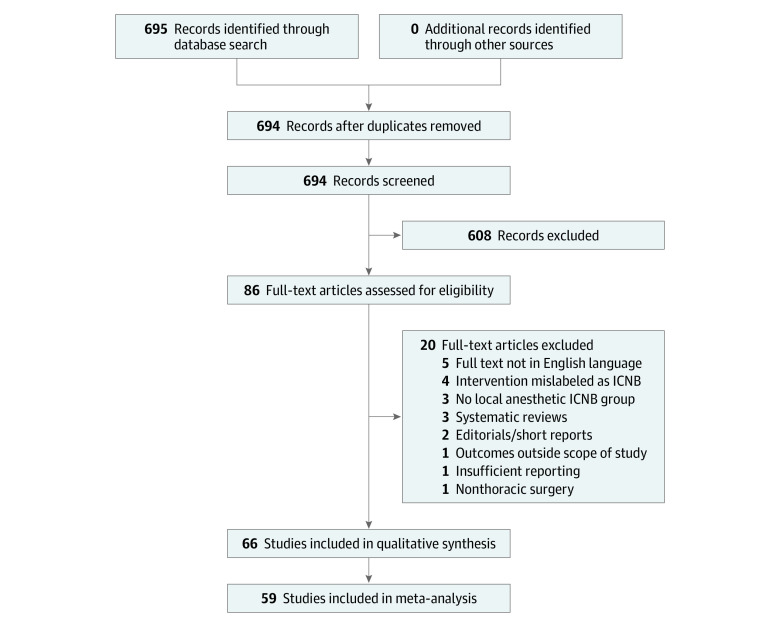
Study selection: Selected studies were experimental or observational and included adult patients undergoing cardiothoracic surgery in which ICNB was administered with local anesthesia via single injection, continuous infusion, or a combination of both techniques in at least 1 group of patients. For comparison with ICNB, studies that examined systemic analgesia and different forms of regional analgesia (such as thoracic epidural analgesia [TEA], paravertebral block [PVB], and other techniques) were included. These criteria were applied independently by 2 authors, and discrepancies were resolved by consensus. A total of 694 records were selected for screening.
Data extraction and synthesis: This study followed the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) reporting guideline. Data including patient characteristics, type of surgery, intervention analgesia, comparison analgesia, and primary and secondary outcomes were extracted independently by 3 authors. Synthesis was performed using a fixed-effects model.
Main outcomes and measures: The coprimary outcomes were postoperative pain intensity (measured as the worst static or dynamic pain using a validated 10-point scale, with 0 indicating no pain and 10 indicating severe pain) and opioid consumption (measured in morphine milligram equivalents [MMEs]) at prespecified intervals (0-6 hours, 7-24 hours, 25-48 hours, 49-72 hours, and >72 hours). Clinically relevant analgesia was defined as a 1-point or greater difference in pain intensity score at any interval. Secondary outcomes included 30-day postoperative complications and pulmonary function.
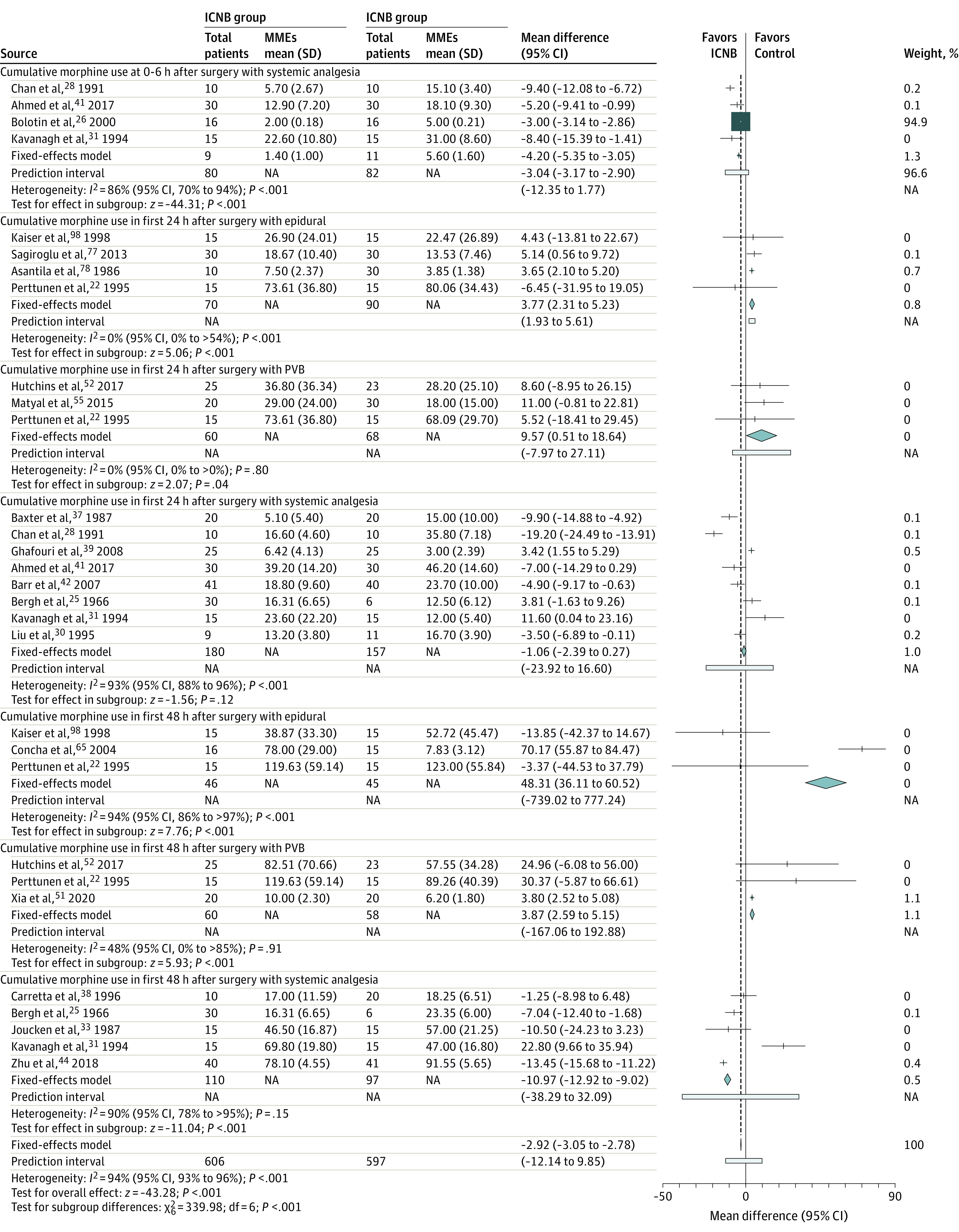
Results: Of 694 records screened, 608 were excluded based on prespecified exclusion criteria. The remaining 86 full-text articles were assessed for eligibility, and 20 of those articles were excluded. All of the 66 remaining studies (5184 patients; mean [SD] age, 53.9 [10.2] years; approximately 59% men and 41% women) were included in the qualitative analysis, and 59 studies (3325 patients) that provided data for at least 1 outcome were included in the quantitative meta-analysis. Experimental studies had a high risk of bias in multiple domains, including allocation concealment, blinding of participants and personnel, and blinding of outcome assessors. Marked differences (eg, crossover studies, timing of the intervention [intraoperative vs postoperative], blinding, and type of control group) were observed in the design and implementation of studies. The use of ICNB vs systemic analgesia was associated with lower static pain (0-6 hours after surgery: mean score difference, -1.40 points [95% CI, -1.46 to -1.33 points]; 7-24 hours after surgery: mean score difference, -1.27 points [95% CI, -1.40 to -1.13 points]) and lower dynamic pain (0-6 hours after surgery: mean score difference, -1.66 points [95% CI, -1.90 to -1.41 points]; 7-24 hours after surgery: mean score difference, -1.43 points [95% CI, -1.70 to -1.17 points]). Intercostal nerve block analgesia was noninferior to TEA (mean score difference in worst dynamic panic at 7-24 hours after surgery: 0.79 points; 95% CI, 0.28-1.29 points) and marginally inferior to PVB (mean score difference in worst dynamic pain at 7-24 hours after surgery: 1.29 points; 95% CI, 1.16 to 1.41 points). The largest opioid-sparing effect of ICNB vs systemic analgesia occurred at 48 hours after surgery (mean difference, -10.97 MMEs; 95% CI, -12.92 to -9.02 MMEs). The use of ICNB was associated with higher MME values compared with TEA (eg, 48 hours after surgery: mean difference, 48.31 MMEs; 95% CI, 36.11-60.52 MMEs) and PVB (eg, 48 hours after surgery: mean difference, 3.87 MMEs; 95% CI, 2.59-5.15 MMEs).
Conclusions and relevance: In this study, single-injection ICNB was associated with a reduction in pain during the first 24 hours after thoracic surgery and was clinically noninferior to TEA or PVB. Intercostal nerve block analgesia had opioid-sparing effects; however, TEA and PVB were associated with larger decreases in postoperative MMEs, suggesting that ICNB may be most beneficial for cases in which TEA and PVB are not indicated.
Conflict of interest statement
Figures
Comment in
-
Chest Wall Analgesia-Where Do We Go From Here?JAMA Netw Open. 2021 Nov 1;4(11):e2133839. doi: 10.1001/jamanetworkopen.2021.33839. JAMA Netw Open. 2021. PMID: 34779854 No abstract available.
References
-
- Bendixen M, Jorgensen OD, Kronborg C, Andersen C, Licht PB. Postoperative pain and quality of life after lobectomy via video-assisted thoracoscopic surgery or anterolateral thoracotomy for early stage lung cancer: a randomised controlled trial. Lancet Oncol. 2016;17(6):836-844. doi: 10.1016/S1470-2045(16)00173-X - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
