

Efficacy of alternative or adjunctive measures to conventional non-surgical and surgical treatment of peri-implant mucositis and peri-implantitis: a systematic review and meta-analysis
- PMID: 34779939
- PMCID: PMC8593130
- DOI: 10.1186/s40729-021-00388-x
Efficacy of alternative or adjunctive measures to conventional non-surgical and surgical treatment of peri-implant mucositis and peri-implantitis: a systematic review and meta-analysis
Abstract
Purpose: To evaluate the efficacy of alternative or adjunctive measures to conventional non-surgical or surgical treatment of peri-implant mucositis and peri-implantitis.
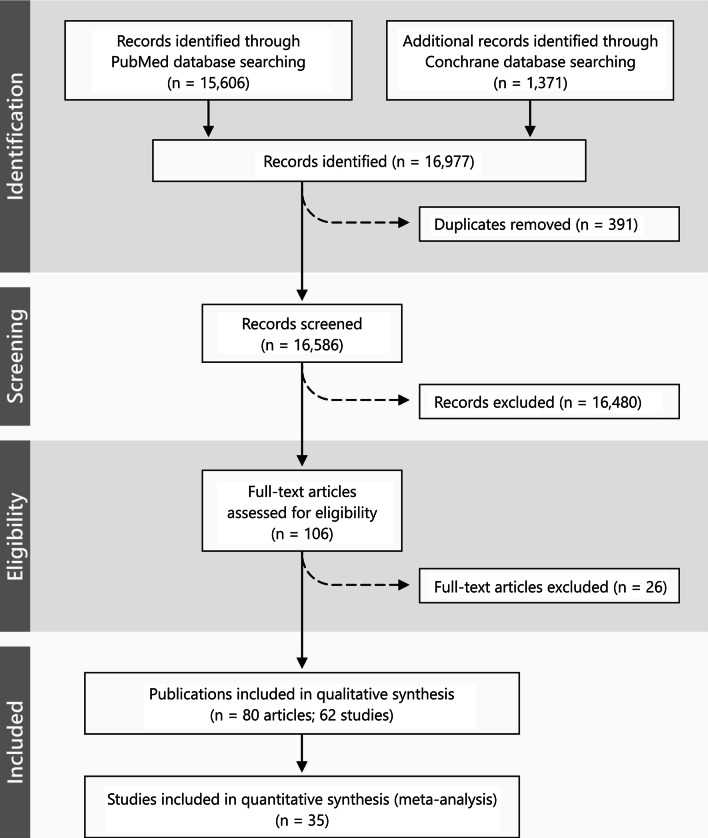
Material and methods: Prospective randomized and nonrandomized controlled studies comparing alternative or adjunctive measures, and reporting on changes in bleeding scores (i.e., bleed0ing index (BI) or bleeding on probing (BOP)), probing depth (PD) values or suppuration (SUPP) were searched.
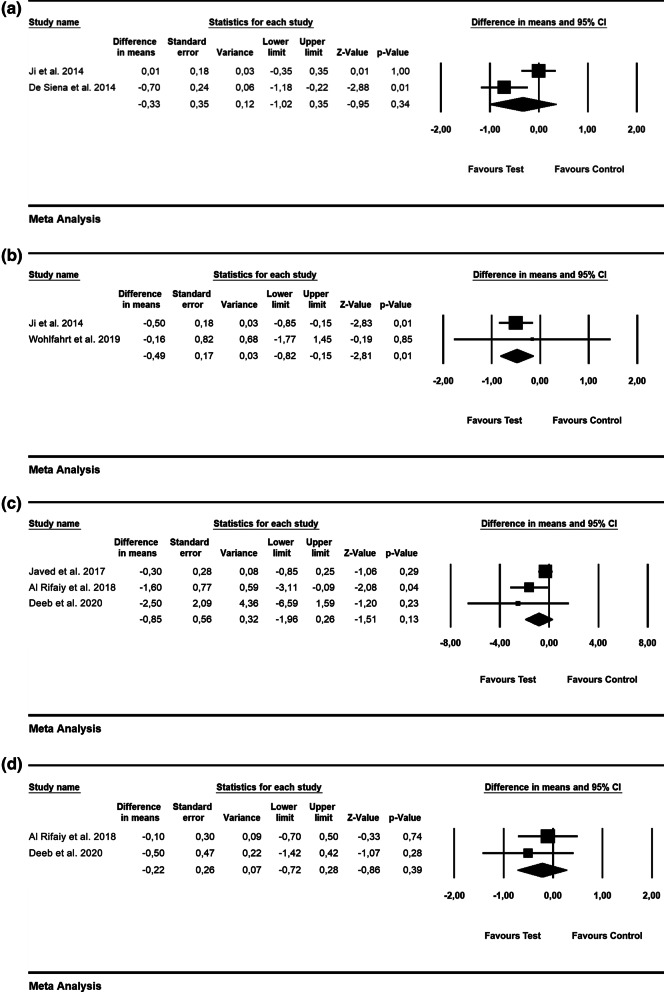
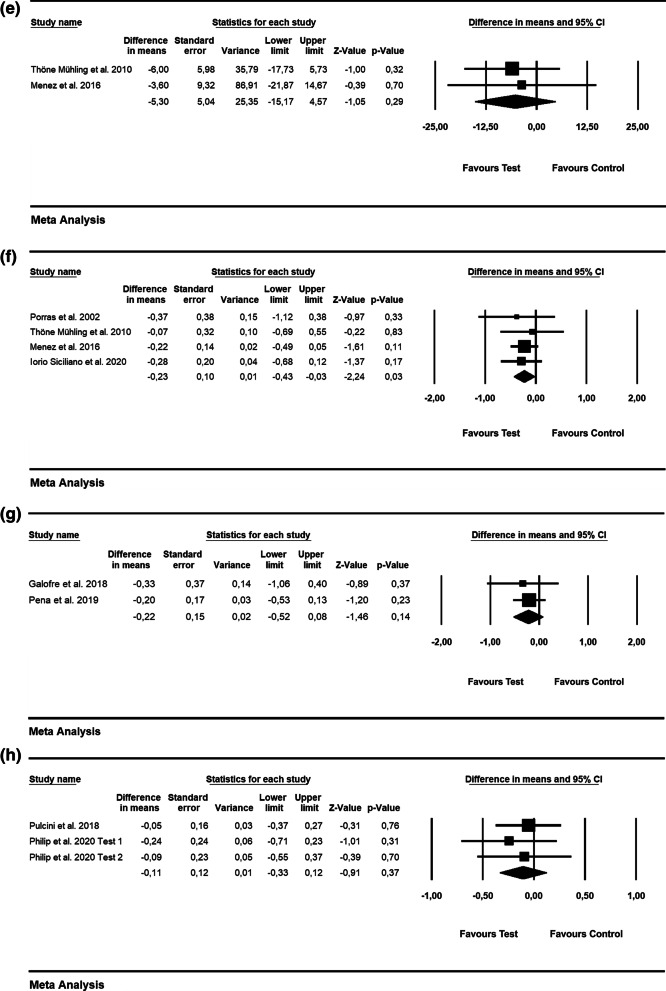
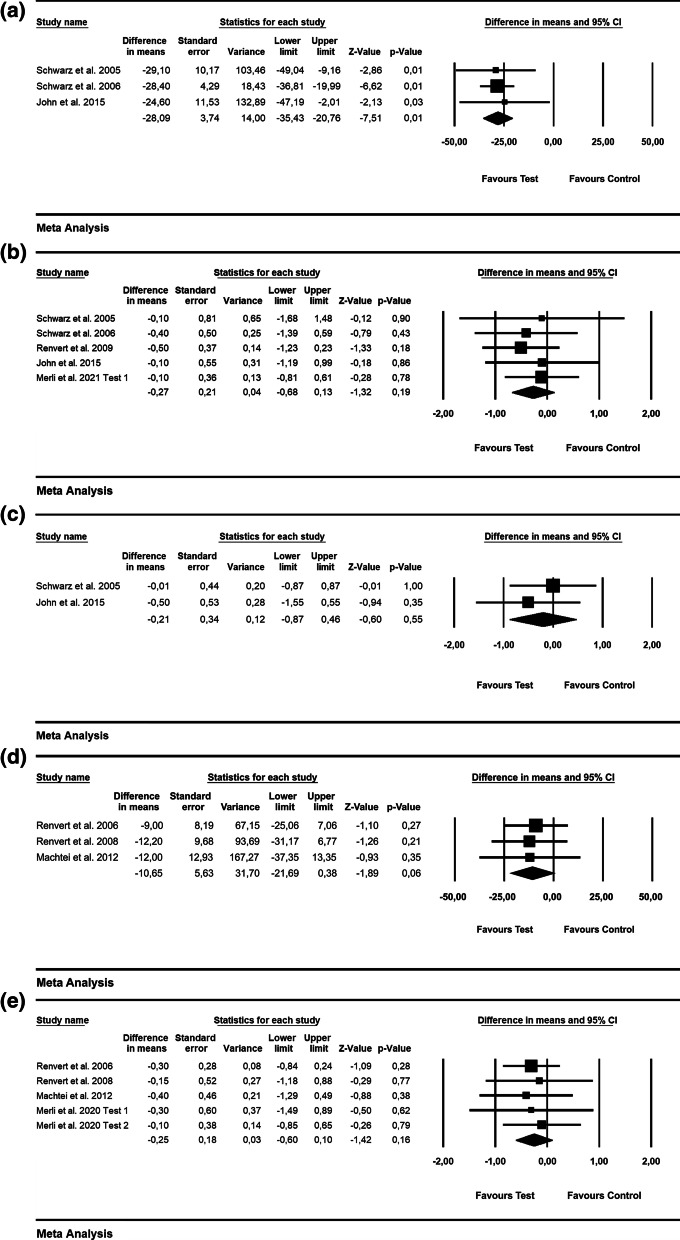
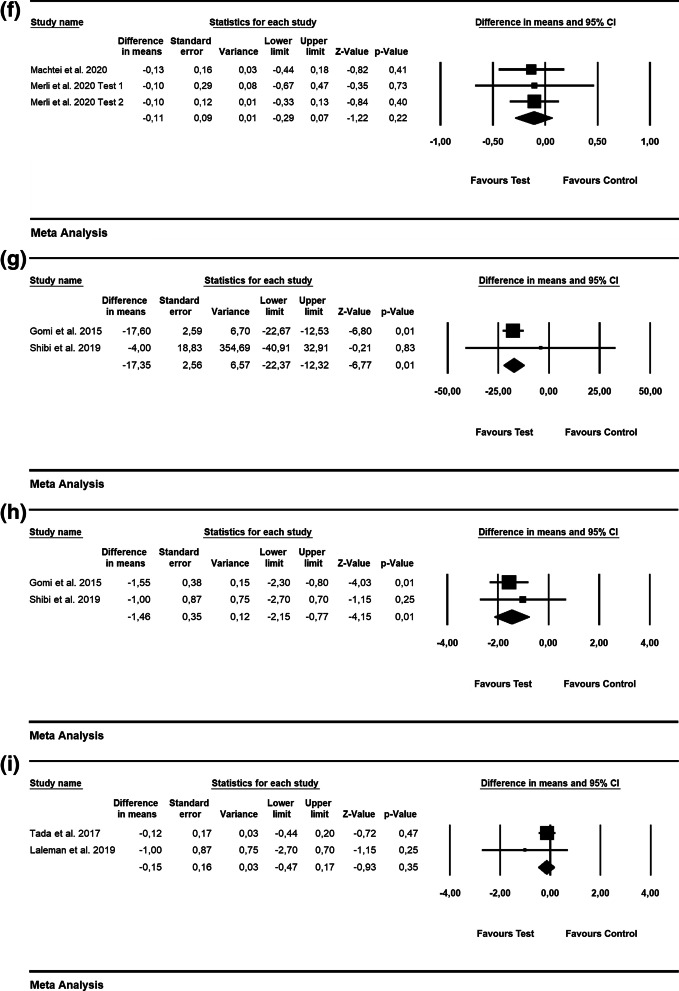
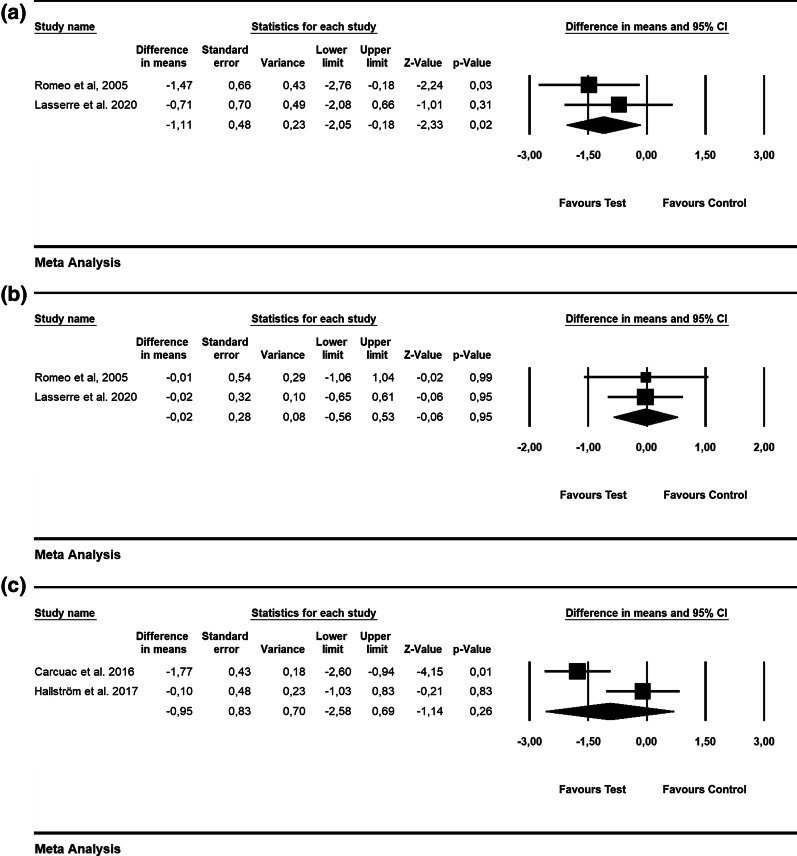
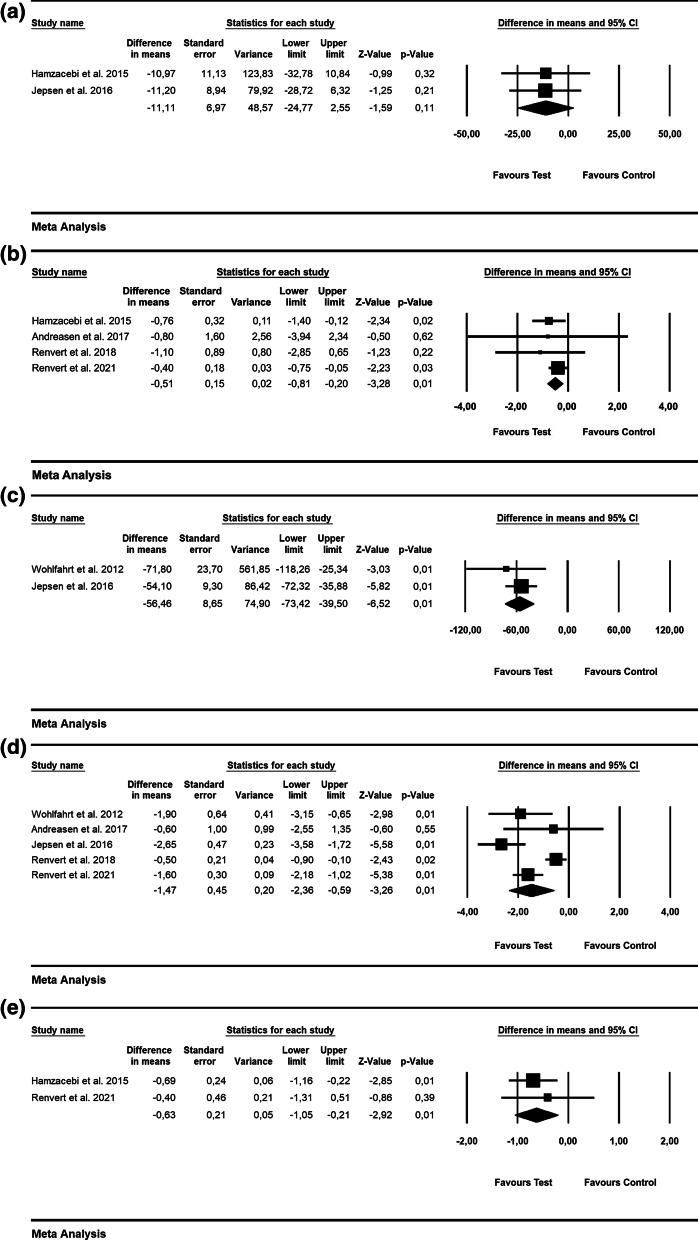
Results: Peri-implant mucositis: adjunctive use of local antiseptics lead to greater PD reduction (weighted mean difference (WMD) = - 0.23 mm; p = 0.03, respectively), whereas changes in BOP were comparable (WMD = - 5.30%; p = 0.29). Non-surgical treatment of peri-implantitis: alternative measures for biofilm removal and systemic antibiotics yielded higher BOP reduction (WMD = - 28.09%; p = 0.01 and WMD = - 17.35%; p = 0.01, respectively). Surgical non-reconstructive peri-implantitis treatment: WMD in PD amounted to - 1.11 mm favoring adjunctive implantoplasty (p = 0.02). Adjunctive reconstructive measures lead to significantly higher radiographic bone defect fill/reduction (WMD = 56.46%; p = 0.01 and WMD = - 1.47 mm; p = 0.01), PD (- 0.51 mm; p = 0.01) and lower soft-tissue recession (WMD = - 0.63 mm; p = 0.01), while changes in BOP were not significant (WMD = - 11.11%; p = 0.11).
Conclusions: Alternative and adjunctive measures provided no beneficial effect in resolving peri-implant mucositis, while alternative measures were superior in reducing BOP values following non-surgical treatment of peri-implantitis. Adjunctive reconstructive measures were beneficial regarding radiographic bone-defect fill/reduction, PD reduction and lower soft-tissue recession, although they did not improve the resolution of mucosal inflammation.
Keywords: Dental implant; Peri-implant disease; Systematic review; Treatment.
© 2021. The Author(s).
Conflict of interest statement
The authors declare that they have no conflict of interests related to this study.
Figures
References
-
- Heitz-Mayfield LJA, Salvi GE. Peri-implant mucositis. J Periodontol. 2018;89(Suppl 1):S257–s266. - PubMed
-
- Berglundh T, et al. Peri-implant diseases and conditions: Consensus report of workgroup 4 of the 2017 World Workshop on the Classification of Periodontal and Peri-Implant Diseases and Conditions. J Clin Periodontol. 2018;45(Suppl 20):S286–s291. - PubMed
-
- Schwarz F, et al. Peri-implantitis. J Periodontol. 2018;89(Suppl 1):S267–s290. - PubMed
-
- Jepsen S, et al. Primary prevention of peri-implantitis: managing peri-implant mucositis. J Clin Periodontol. 2015;42(Suppl 16):S152–S157. - PubMed
-
- Derks J, et al. Peri-implantitis - onset and pattern of progression. J Clin Periodontol. 2016;43(4):383–388. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
