

European Stroke Organisation (ESO) guidelines on blood pressure management in acute ischaemic stroke and intracerebral haemorrhage
- PMID: 34780578
- PMCID: PMC8370078
- DOI: 10.1177/23969873211012133
European Stroke Organisation (ESO) guidelines on blood pressure management in acute ischaemic stroke and intracerebral haemorrhage
Abstract
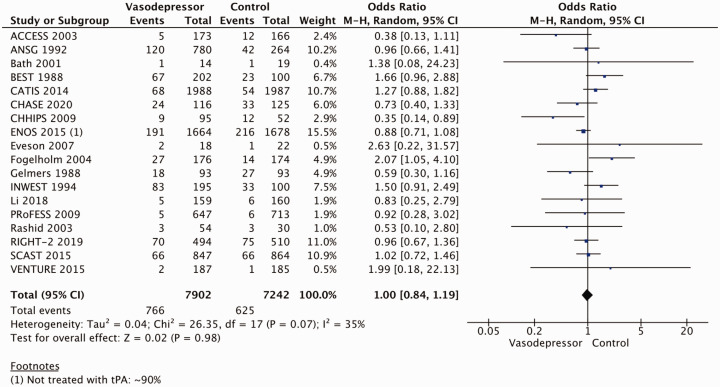
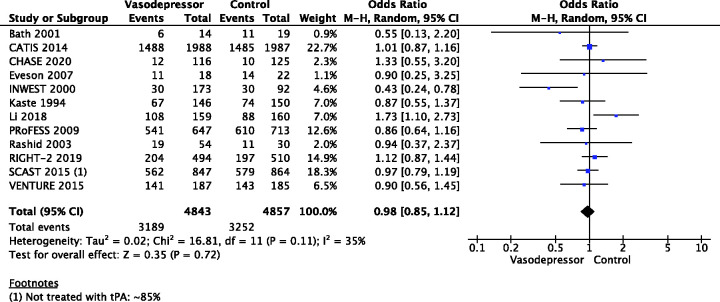
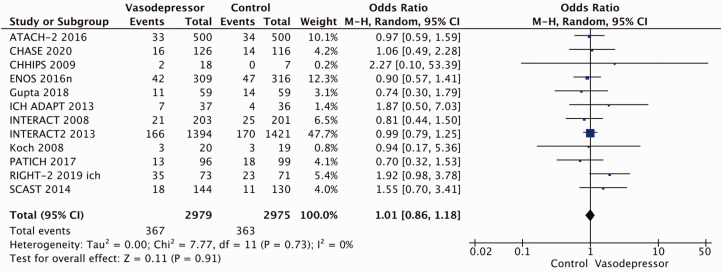
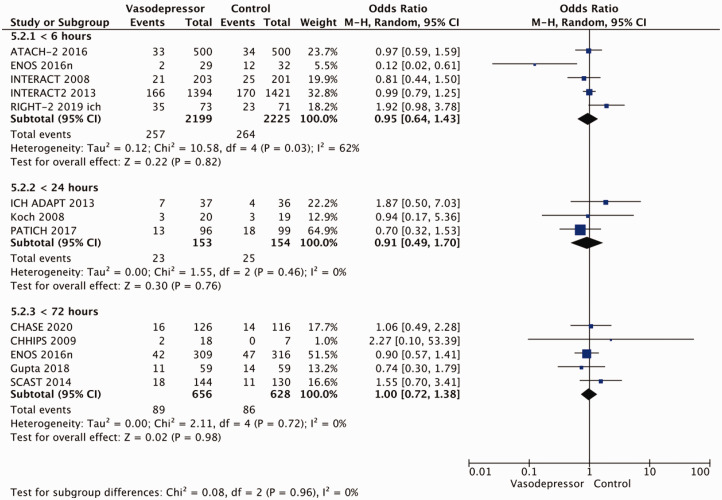
The optimal blood pressure (BP) management in acute ischaemic stroke (AIS) and acute intracerebral haemorrhage (ICH) remains controversial. These European Stroke Organisation (ESO) guidelines provide evidence-based recommendations to assist physicians in their clinical decisions regarding BP management in acute stroke.The guidelines were developed according to the ESO standard operating procedure and Grading of Recommendations, Assessment, Development, and Evaluation (GRADE) methodology. The working group identified relevant clinical questions, performed systematic reviews and meta-analyses of the literature, assessed the quality of the available evidence, and made specific recommendations. Expert consensus statements were provided where insufficient evidence was available to provide recommendations based on the GRADE approach. Despite several large randomised-controlled clinical trials, quality of evidence is generally low due to inconsistent results of the effect of blood pressure lowering in AIS. We recommend early and modest blood pressure control (avoiding blood pressure levels >180/105 mm Hg) in AIS patients undergoing reperfusion therapies. There is more high-quality randomised evidence for BP lowering in acute ICH, where intensive blood pressure lowering is recommended rapidly after hospital presentation with the intent to improve recovery by reducing haematoma expansion. These guidelines provide further recommendations on blood pressure thresholds and for specific patient subgroups. There is ongoing uncertainty regarding the most appropriate blood pressure management in AIS and ICH. Future randomised-controlled clinical trials are needed to inform decision making on thresholds, timing and strategy of blood pressure lowering in different acute stroke patient subgroups.
Keywords: antihypertensive; blood pressure; blood pressure lowering; guidelines; hypertension; intracerebral haemorrhage; ischaemic stroke; recommendations.
© European Stroke Organisation 2021.
Conflict of interest statement
Declaration of conflicting interests: Declarations of conflicts of interests are outlined in table 1.
Figures






References
-
- Bath PM, Appleton JP, Krishnan K, et al.. Blood pressure in acute stroke: to treat or not to treat: that is still the question. Stroke 2018; 49: 1784–1790. - PubMed
-
- Carcel C, Anderson CS.Timing of blood pressure lowering in acute ischemic stroke. Curr Atheroscler Rep 2015; 17: 42. - PubMed
-
- Jusufovic M, Mishra NK, Lansberg MG, et al.. Blood pressure management in acute stroke. Curr Hypertens Rev 2016; 12: 121–126. - PubMed
-
- Qureshi AI.Acute hypertensive response in patients with stroke: pathophysiology and management. Circulation 2008; 118: 176–187. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
