

Integrative Analysis of the Inflammatory Bowel Disease Serum Metabolome Improves Our Understanding of Genetic Etiology and Points to Novel Putative Therapeutic Targets
- PMID: 34780722
- PMCID: PMC9214725
- DOI: 10.1053/j.gastro.2021.11.015
Integrative Analysis of the Inflammatory Bowel Disease Serum Metabolome Improves Our Understanding of Genetic Etiology and Points to Novel Putative Therapeutic Targets
Abstract
Background & aims: Polygenic and environmental factors are underlying causes of inflammatory bowel disease (IBD). We hypothesized that integration of the genetic loci controlling a metabolite's abundance, with known IBD genetic susceptibility loci, may help resolve metabolic drivers of IBD.
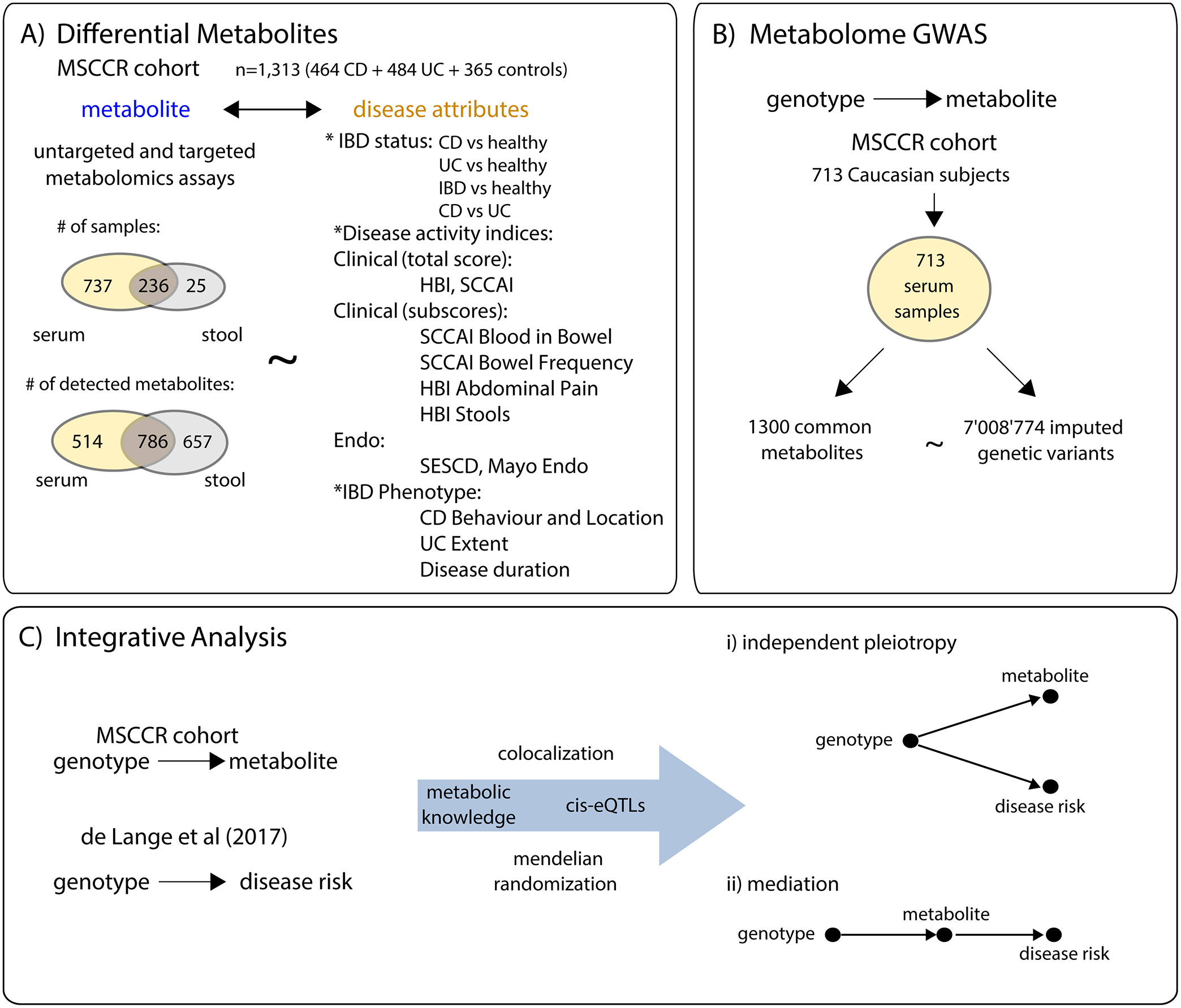
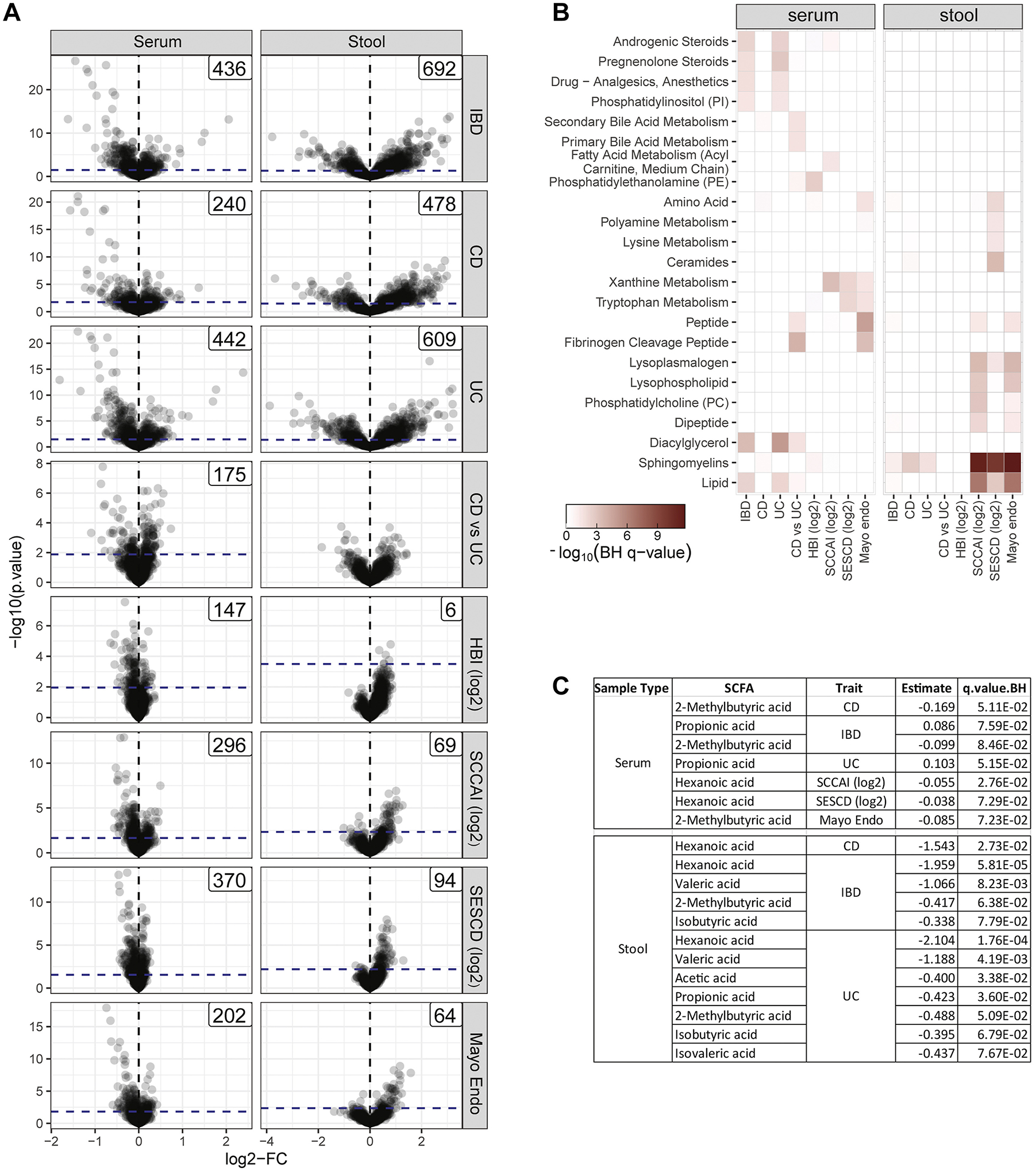
Methods: We measured the levels of 1300 metabolites in the serum of 484 patients with ulcerative colitis (UC) and 464 patients with Crohn's disease (CD) and 365 controls. Differential metabolite abundance was determined for disease status, subtype, clinical and endoscopic disease activity, as well as IBD phenotype including disease behavior, location, and extent. To inform on the genetic basis underlying metabolic diversity, we integrated metabolite and genomic data. Genetic colocalization and Mendelian randomization analyses were performed using known IBD risk loci to explore whether any metabolite was causally associated with IBD.
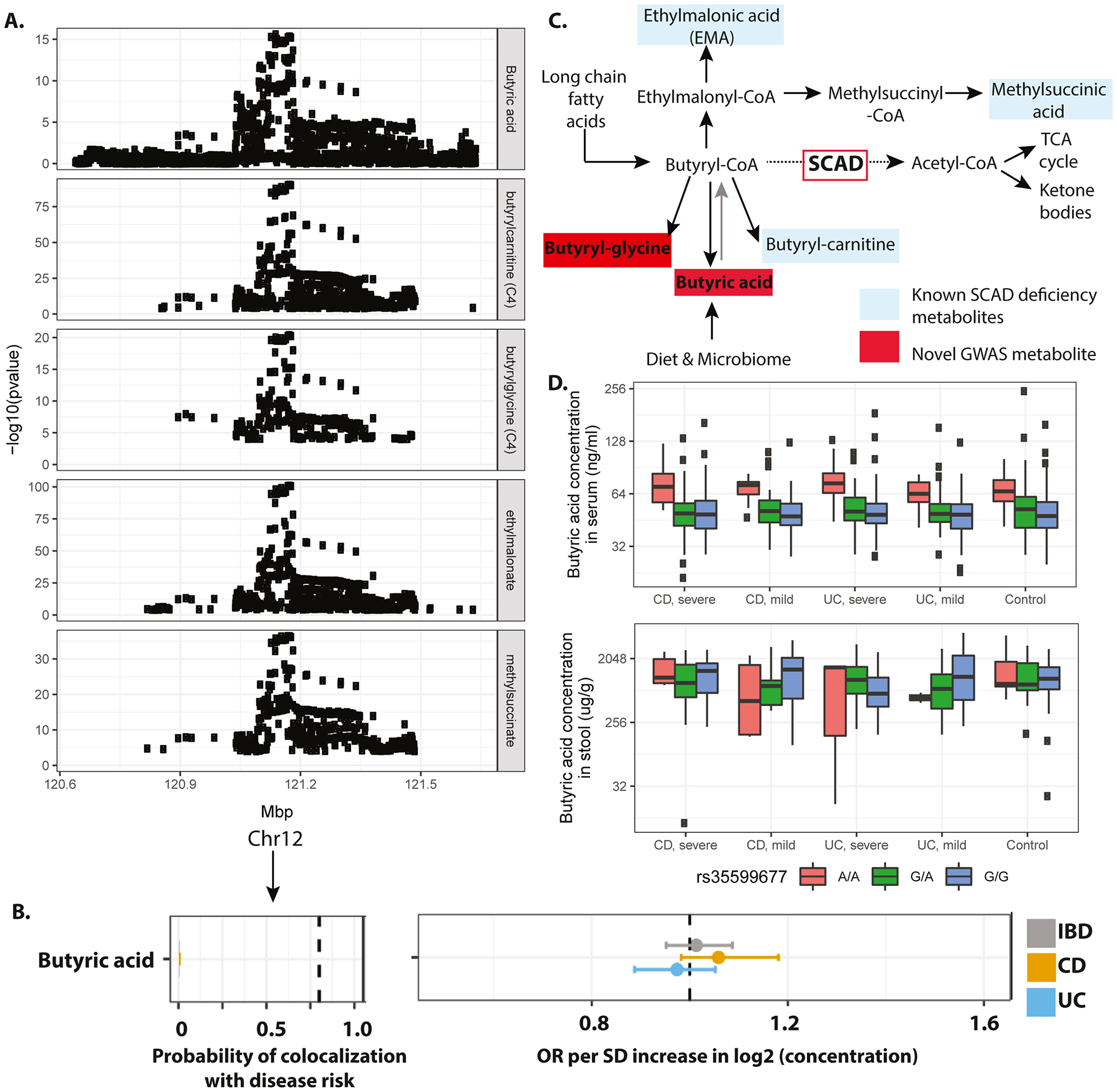
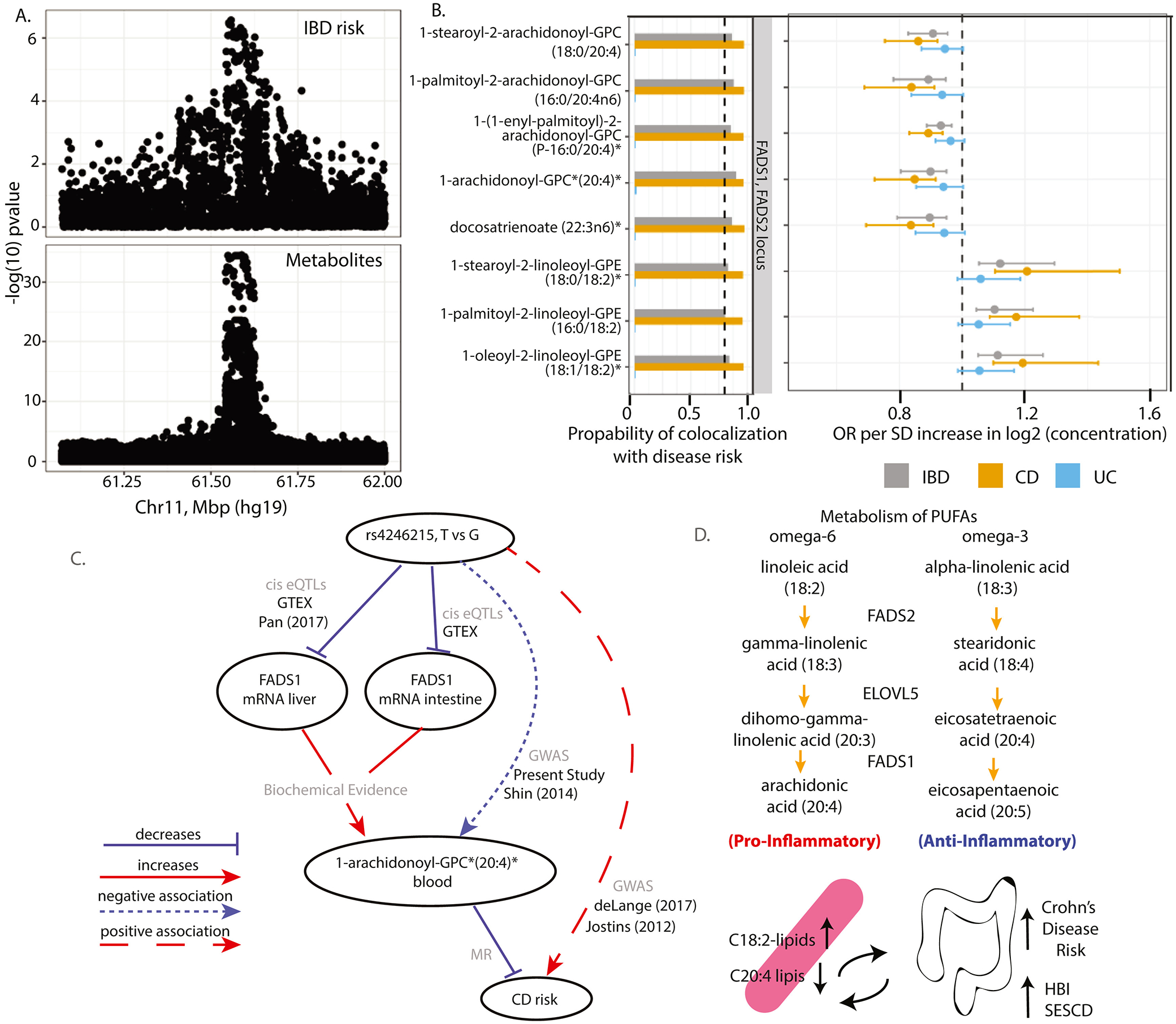
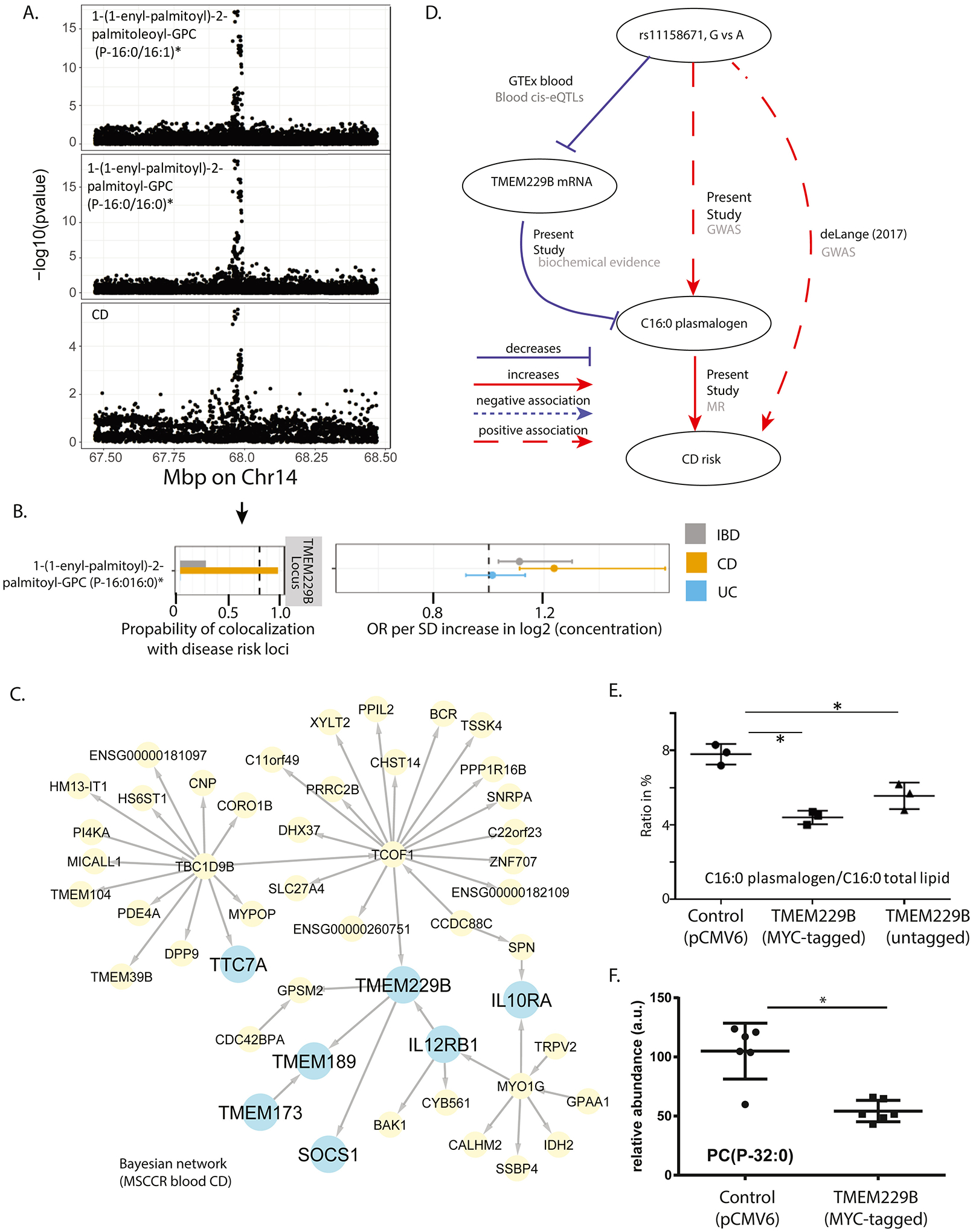
Results: We found 173 genetically controlled metabolites (metabolite quantitative trait loci, 9 novel) within 63 non-overlapping loci (7 novel). Furthermore, several metabolites significantly associated with IBD disease status and activity as defined using clinical and endoscopic indexes. This constitutes a resource for biomarker discovery and IBD biology insights. Using this resource, we show that a novel metabolite quantitative trait locus for serum butyrate levels containing ACADS was not supported as causal for IBD; replicate the association of serum omega-6 containing lipids with the fatty acid desaturase 1/2 locus and identify these metabolites as causal for CD through Mendelian randomization; and validate a novel association of serum plasmalogen and TMEM229B, which was predicted as causal for CD.
Conclusions: An exploratory analysis combining genetics and unbiased serum metabolome surveys can reveal novel biomarkers of disease activity and potential mediators of pathology in IBD.
Keywords: Differential Metabolite Abundance Analysis; Inflammatory Bowel Disease; Mendelian Randomization; Metabolome.
Copyright © 2022 AGA Institute. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Ng SC et al. Worldwide incidence and prevalence of inflammatory bowel disease in the 21st century: a systematic review of population-based studies. Lancet 390, 2769–2778 (2018). - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
