

Tacrolimus-induced neurotoxicity from bipolar disorder to status epilepticus under the therapeutic serum level: a case report
- PMID: 34781882
- PMCID: PMC8591960
- DOI: 10.1186/s12883-021-02479-z
Tacrolimus-induced neurotoxicity from bipolar disorder to status epilepticus under the therapeutic serum level: a case report
Abstract
Background: Tacrolimus is a macrolide immunosuppressant widely used to prevent rejection after solid organ transplantation. In general, adverse events of tacrolimus occur more often as the concentration of tacrolimus in the blood increases. We report the case of a 39-year-old man who developed a variety of adverse events despite in the therapeutic level of tacrolimus in the blood.
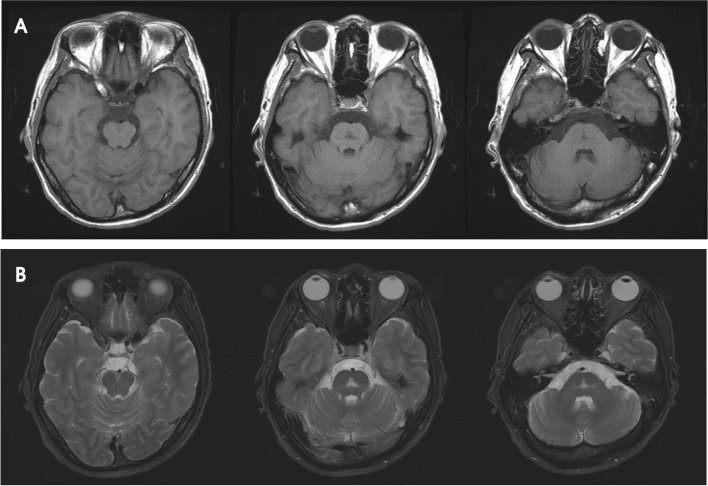
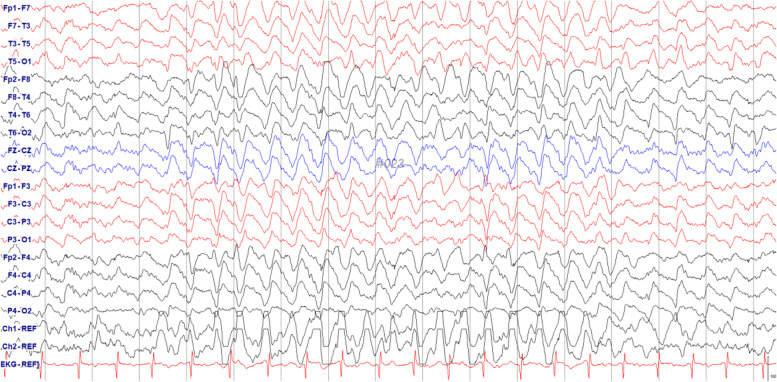
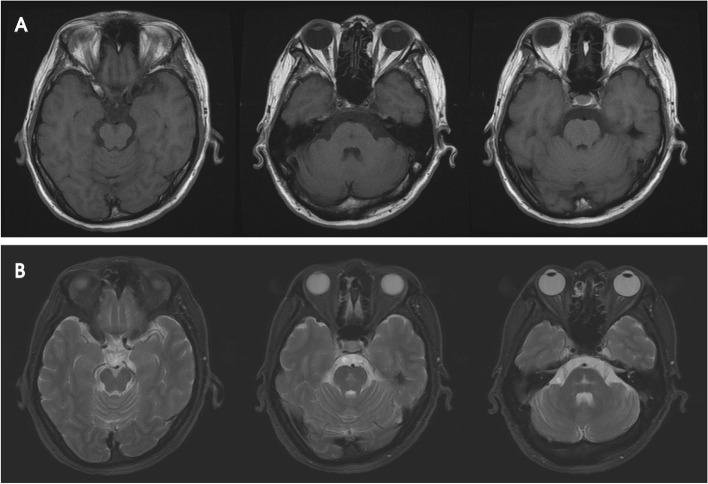
Case presentation: A 39-year-old man underwent liver transplantation for liver cirrhosis due to alcoholic liver disease. The postoperative immunosuppressant consisted of tacrolimus (5 mg) and mycophenolate (500 mg) twice daily. Five months after taking tacrolimus, he presented with talkativeness, which gradually worsened. Brain magnetic resonance imaging performed 10 months after tacrolimus administration revealed a hyperintense lesion affecting the middle of the pontine tegmentum on T2WI. The blood concentration of tacrolimus was 7.2 ng/mL (therapeutic range 5-20 ng/mL). After 21 months, he exhibited postural tremor in both the hands. Twenty-four months after taking tacrolimus, he showed drowsy mentality, intention tremor, and dysdiadochokinesia. Electroencephalography presented generalized high-voltage rhythmic delta waves; therefore, tacrolimus was discontinued in suspicion of tacrolimus-induced neurotoxicity, and anticonvulsive treatment was started. The level of consciousness gradually improved, and the patient was able to walk independently with mild ataxia.
Conclusion: This case shows that tacrolimus-induced neurotoxicity can occur even at normal concentrations. Therefore, if a patient taking tacrolimus exhibits psychiatric or neurologic symptoms, neurotoxicity should be considered even when the blood tacrolimus is within the therapeutic range.
Keywords: Ataxia; Bipolar disorder; Neurotoxicity; Status epilepticus; Tacrolimus.
© 2021. The Author(s).
Conflict of interest statement
The authors declare that there are no conflicts of interest.
Figures

References
-
- Trouillas P, Takayanagi T, Hallett M, et al. International cooperative ataxia rating scale for pharmacological assessment of the cerebellar syndrome. The Ataxia neuropharmacology Committee of the World Federation of neurology. J Neurol Sci. 1997;145:205–211. doi: 10.1016/S0022-510X(96)00231-6. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
