

Eight-year post-trial follow-up of morbidity and mortality of telephone health coaching
- PMID: 34781936
- PMCID: PMC8594149
- DOI: 10.1186/s12913-021-07263-w
Eight-year post-trial follow-up of morbidity and mortality of telephone health coaching
Abstract
Background: Health coaching is a patient-centred approach to supporting self-management for the chronic conditions. However, long-term evidence of effectiveness of health coaching remains scarce. The object of this study was to evaluate the long-term effect of telephone health coaching (THC) on mortality and morbidity among people with type 2 diabetes (T2D), coronary artery disease (CAD) and congestive heart failure (CHF)..
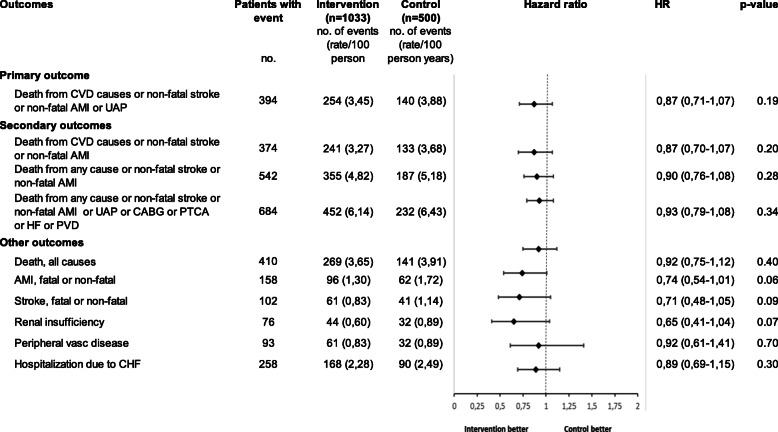
Methods: 1535 T2D, CAD and CHF patients with unmet treatment targets were randomly allocated into an intervention group (n = 1034) and control group (n = 501). Intervention group received monthly individual strength-based, autonomy supportive THC sessions (average 30 min) for behavior change with a specially trained nurse for 12 months additional to usual health care. Control group received usual health care services. The primary outcome was a composite of death from cardiovascular causes or non-fatal stroke or non-fatal myocardial infarction (AMI) or unstable angina pectoris (UAP) during a follow-up of 8 years Three other composite endpoints with distinct combinations of fatal and non-fatal cardiovascular events and death from any cause were used as secondary outcomes. Other outcomes followed were the most relevant components of the composite endpoints. Randomized controlled trial (RCT) data was linked to Finnish national health and social care registries and electronic health records (EHR). Post-trial eight-year evaluation was conducted using intention-to-treat (ITT) and per-protocol (PP) analysis.
Results: The composite primary outcome event rate per 100 person years was lower in the intervention group (3.45) than in control group (3.88) in ITT -analysis, but the difference was not statistically significant (hazard ratio in the intervention group 0.87; 95% CI, 0.71 to 1.07; P = 0.19). In the subgroup (T2D, CAD/CHF) analysis, there were no statistically significant effects. The secondary PP-analysis showed statistically significant benefits for those who participated in the study.
Conclusions: No statistically significant effect of health coaching on mortality and morbidity was found in intention to treat analysis. The per protocol results suggest, however, that the intervention may be effective among patients who are willing and able to participate in health coaching. More research is needed to identify patients most likely to benefit from low-intensity health coaching.
Trial registration: NCT00552903 (registration date: the 1st of November 2007, updated the 3rd of February 2009).
Keywords: Coronary artery disease; Health coaching; Morbidity; Mortality; Type 2 diabetes.
© 2021. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interest.
Figures

References
-
- Eurostat 2014. https://ec.europa.eu/eurostat/ (Accessed May 27, 2020).
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
