

SARS-CoV-2 involvement in central nervous system tissue damage
- PMID: 34782556
- PMCID: PMC8643043
- DOI: 10.4103/1673-5374.327323
SARS-CoV-2 involvement in central nervous system tissue damage
Abstract
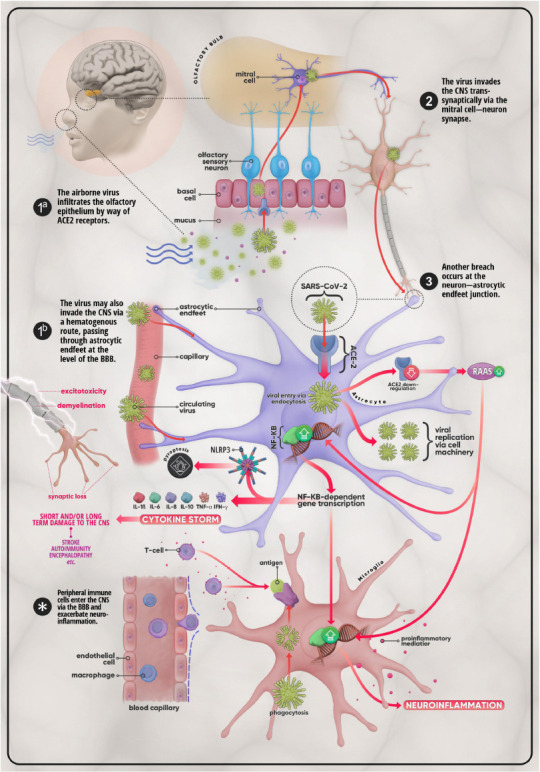
As the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) continues to spread globally, it became evident that the SARS-CoV-2 virus infects multiple organs including the brain. Several clinical studies revealed that patients with COVID-19 infection experience an array of neurological signs ranging in severity from headaches to life-threatening strokes. Although the exact mechanism by which the SARS-CoV-2 virus directly impacts the brain is not fully understood, several theories have been suggested including direct and indirect pathways induced by the virus. One possible theory is the invasion of SARS-CoV-2 to the brain occurs either through the bloodstream or via the nerve endings which is considered to be the direct route. Such findings are based on studies reporting the presence of viral material in the cerebrospinal fluid and brain cells. Nevertheless, the indirect mechanisms, including blood-clotting abnormalities and prolonged activation of the immune system, can result in further tissue and organ damages seen during the course of the disease. This overview attempts to give a thorough insight into SARS-CoV-2 coronavirus neurological infection and highlights the possible mechanisms leading to the neurological manifestations observed in infected patients.
Keywords: CNS infection; COVID-19; autoantibodies; coagulopathy; encephalitis; neuroinflammation; renin-angiotensin system; viral encephalopathy.
Conflict of interest statement
None
Figures
References
-
- Al Saiegh F, Ghosh R, Leibold A, Avery MB, Schmidt RF, Theofanis T, Mouchtouris N, Philipp L, Peiper SC, Wang ZX, Rincon F, Tjoumakaris SI, Jabbour P, Rosenwasser RH, Gooch MR. Status of SARS-CoV-2 in cerebrospinal fluid of patients with COVID-19 and stroke. J Neurol Neurosurg Psychiatry. 2020;91:846–848. - PubMed
-
- Amraie R, Napoleon MA, Yin W, Berrigan J, Suder E, Zhao G, Olejnik J, Gummuluru S, Muhlberger E, Chitalia V, Rahimi N. CD209L/L-SIGN and CD209/DC-SIGN act as receptors for SARS-CoV-2 and are differentially expressed in lung and kidney epithelial and endothelial cells. bioRxiv. 2020. doi:10.1101/2020.06.22.165803. Available from: https://www.biorxiv.org/content/10.1101/2020.06.22.165803v3 .
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
