

Consumption of coffee and tea and risk of developing stroke, dementia, and poststroke dementia: A cohort study in the UK Biobank
- PMID: 34784347
- PMCID: PMC8594796
- DOI: 10.1371/journal.pmed.1003830
Consumption of coffee and tea and risk of developing stroke, dementia, and poststroke dementia: A cohort study in the UK Biobank
Abstract
Background: Previous studies have revealed the involvement of coffee and tea in the development of stroke and dementia. However, little is known about the association between the combination of coffee and tea and the risk of stroke, dementia, and poststroke dementia. Therefore, we aimed to investigate the associations of coffee and tea separately and in combination with the risk of developing stroke and dementia.
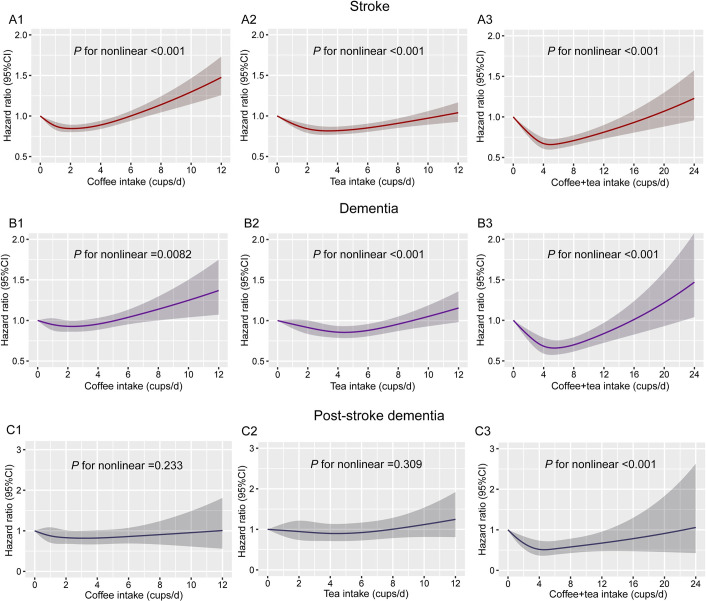
Methods and findings: This prospective cohort study included 365,682 participants (50 to 74 years old) from the UK Biobank. Participants joined the study from 2006 to 2010 and were followed up until 2020. We used Cox proportional hazards models to estimate the associations between coffee/tea consumption and incident stroke and dementia, adjusting for sex, age, ethnicity, qualification, income, body mass index (BMI), physical activity, alcohol status, smoking status, diet pattern, consumption of sugar-sweetened beverages, high-density lipoprotein (HDL), low-density lipoprotein (LDL), history of cancer, history of diabetes, history of cardiovascular arterial disease (CAD), and hypertension. Coffee and tea consumption was assessed at baseline. During a median follow-up of 11.4 years for new onset disease, 5,079 participants developed dementia, and 10,053 participants developed stroke. The associations of coffee and tea with stroke and dementia were nonlinear (P for nonlinear <0.01), and coffee intake of 2 to 3 cups/d or tea intake of 3 to 5 cups/d or their combination intake of 4 to 6 cups/d were linked with the lowest hazard ratio (HR) of incident stroke and dementia. Compared with those who did not drink tea and coffee, drinking 2 to 3 cups of coffee and 2 to 3 cups of tea per day was associated with a 32% (HR 0.68, 95% CI, 0.59 to 0.79; P < 0.001) lower risk of stroke and a 28% (HR, 0.72, 95% CI, 0.59 to 0.89; P = 0.002) lower risk of dementia. Moreover, the combination of coffee and tea consumption was associated with lower risk of ischemic stroke and vascular dementia. Additionally, the combination of tea and coffee was associated with a lower risk of poststroke dementia, with the lowest risk of incident poststroke dementia at a daily consumption level of 3 to 6 cups of coffee and tea (HR, 0.52, 95% CI, 0.32 to 0.83; P = 0.007). The main limitations were that coffee and tea intake was self-reported at baseline and may not reflect long-term consumption patterns, unmeasured confounders in observational studies may result in biased effect estimates, and UK Biobank participants are not representative of the whole United Kingdom population.
Conclusions: We found that drinking coffee and tea separately or in combination were associated with lower risk of stroke and dementia. Intake of coffee alone or in combination with tea was associated with lower risk of poststroke dementia.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures


References
-
- Iadecola C, Duering M, Hachinski V, Joutel A, Pendlebury ST, Schneider JA, et al. Vascular Cognitive Impairment and Dementia: JACC Scientific Expert Panel. J Am Coll Cardiol 2019;73(25):3326–44. Epub 2019/06/30. doi: 10.1016/j.jacc.2019.04.034 ; PubMed Central PMCID: PMC6719789. - DOI - PMC - PubMed
-
- International AsD. World Alzheimer’s Report 2019. Available at: https://www.alz.co.uk/research/world-report-2019.
-
- Collaborators GBDCoD. Global, regional, and national age-sex specific mortality for 264 causes of death, 1980–2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet 2017;390(10100):1151–210. Epub 2017/09/19. doi: 10.1016/S0140-6736(17)32152-9 ; PubMed Central PMCID: PMC5605883. - DOI - PMC - PubMed
-
- Disease GBD, Injury I, Prevalence C. Global, regional, and national incidence, prevalence, and years lived with disability for 310 diseases and injuries, 1990–2015: a systematic analysis for the Global Burden of Disease Study 2015. Lancet 2016;388(10053):1545–602. Epub 2016/10/14. doi: 10.1016/S0140-6736(16)31678-6 ; PubMed Central PMCID: PMC5055577. - DOI - PMC - PubMed
-
- Feigin VL, Krishnamurthi RV, Parmar P, Norrving B, Mensah GA, Bennett DA, et al. Update on the Global Burden of Ischemic and Hemorrhagic Stroke in 1990–2013: The GBD 2013 Study. Neuroepidemiology 2015;45(3):161–76. Epub 2015/10/28. doi: 10.1159/000441085 ; PubMed Central PMCID: PMC4633282. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
