

Selective identification and localization of indolent and aggressive prostate cancers via CorrSigNIA: an MRI-pathology correlation and deep learning framework
- PMID: 34784540
- PMCID: PMC8678366
- DOI: 10.1016/j.media.2021.102288
Selective identification and localization of indolent and aggressive prostate cancers via CorrSigNIA: an MRI-pathology correlation and deep learning framework
Abstract
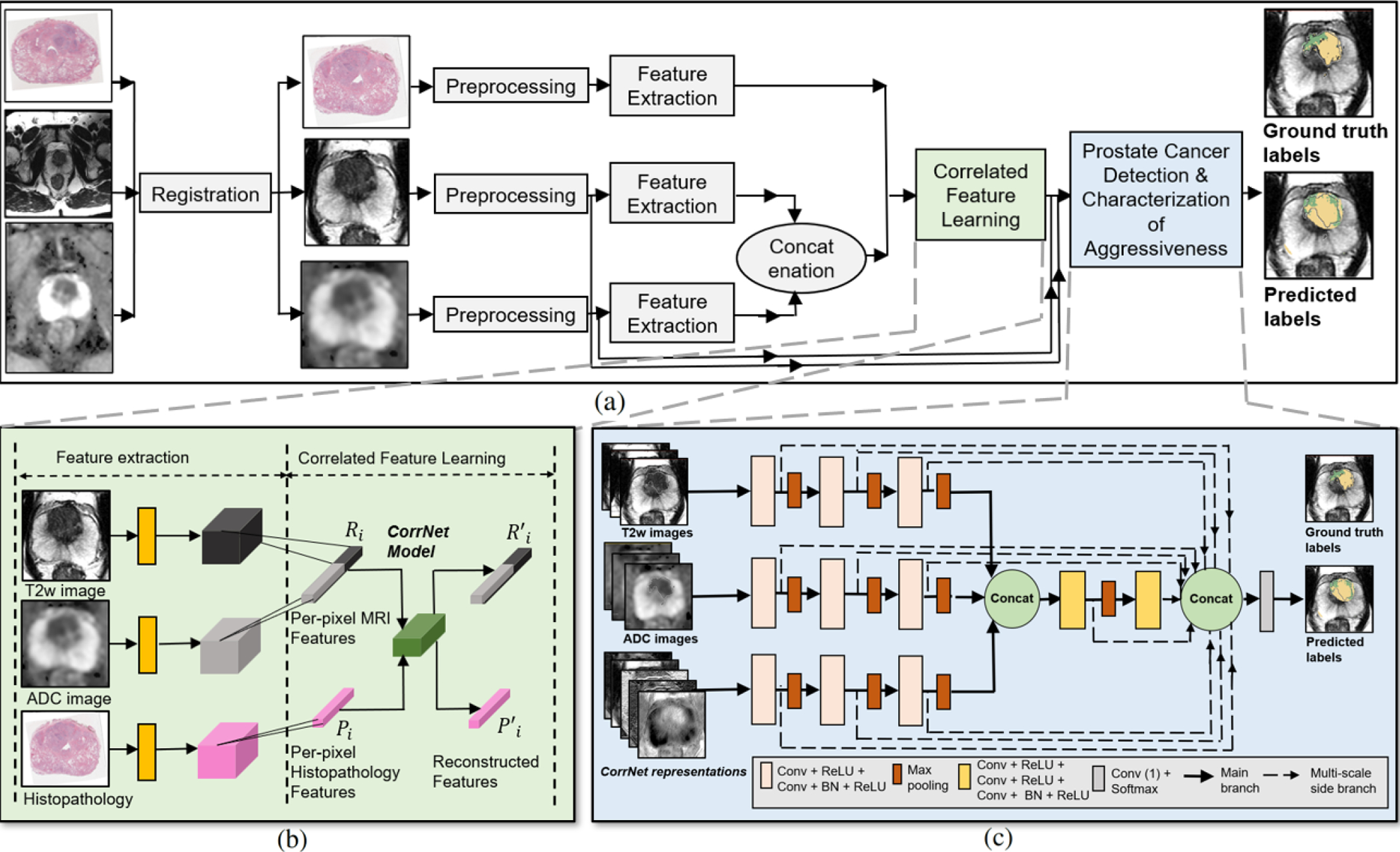
Automated methods for detecting prostate cancer and distinguishing indolent from aggressive disease on Magnetic Resonance Imaging (MRI) could assist in early diagnosis and treatment planning. Existing automated methods of prostate cancer detection mostly rely on ground truth labels with limited accuracy, ignore disease pathology characteristics observed on resected tissue, and cannot selectively identify aggressive (Gleason Pattern≥4) and indolent (Gleason Pattern=3) cancers when they co-exist in mixed lesions. In this paper, we present a radiology-pathology fusion approach, CorrSigNIA, for the selective identification and localization of indolent and aggressive prostate cancer on MRI. CorrSigNIA uses registered MRI and whole-mount histopathology images from radical prostatectomy patients to derive accurate ground truth labels and learn correlated features between radiology and pathology images. These correlated features are then used in a convolutional neural network architecture to detect and localize normal tissue, indolent cancer, and aggressive cancer on prostate MRI. CorrSigNIA was trained and validated on a dataset of 98 men, including 74 men that underwent radical prostatectomy and 24 men with normal prostate MRI. CorrSigNIA was tested on three independent test sets including 55 men that underwent radical prostatectomy, 275 men that underwent targeted biopsies, and 15 men with normal prostate MRI. CorrSigNIA achieved an accuracy of 80% in distinguishing between men with and without cancer, a lesion-level ROC-AUC of 0.81±0.31 in detecting cancers in both radical prostatectomy and biopsy cohort patients, and lesion-levels ROC-AUCs of 0.82±0.31 and 0.86±0.26 in detecting clinically significant cancers in radical prostatectomy and biopsy cohort patients respectively. CorrSigNIA consistently outperformed other methods across different evaluation metrics and cohorts. In clinical settings, CorrSigNIA may be used in prostate cancer detection as well as in selective identification of indolent and aggressive components of prostate cancer, thereby improving prostate cancer care by helping guide targeted biopsies, reducing unnecessary biopsies, and selecting and planning treatment.
Keywords: Computer-aided diagnosis; Correlated feature learning; Prostate cancer; Radiology-pathology fusion.
Copyright © 2021 The Authors. Published by Elsevier B.V. All rights reserved.
Conflict of interest statement
Declaration of Competing Interest The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures

References
-
- Abraham B, Nair MS, 2019. Automated grading of prostate cancer using convolutional neural network and ordinal class classifier. Informatics in Medicine Unlocked 17, 100256.
-
- Ahmed HU, Bosaily AES, Brown LC, Gabe R, Kaplan R, Parmar MK, Collaco-Moraes Y, Ward K, Hindley RG, Freeman A, et al., 2017. Diagnostic accuracy of multi-parametric MRI and TRUS biopsy in prostate cancer (PROMIS): A paired validating confirmatory study. The Lancet 389, 815–822. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
