

Thromboembolism and bleeding in systemic amyloidosis: a review
- PMID: 34784656
- PMCID: PMC8787981
- DOI: 10.1002/ehf2.13701
Thromboembolism and bleeding in systemic amyloidosis: a review
Abstract
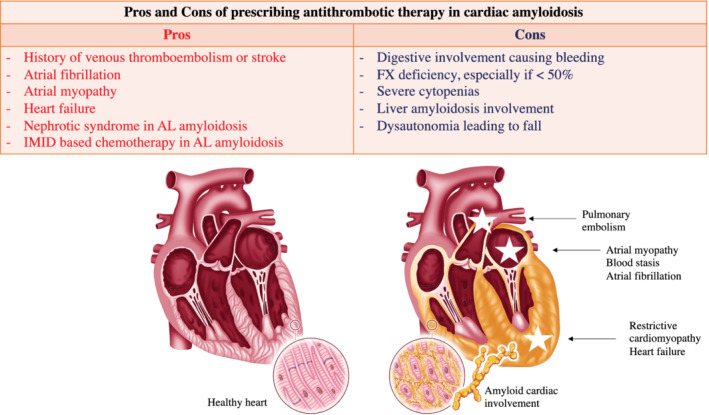
The assessment of both thromboembolic and haemorrhagic risks and their management in systemic amyloidosis have been poorly emphasized so far. This narrative review summarizes main evidence from literature with clinical perspective. The rate of thromboembolic events is as high as 5-10% amyloidosis patients, at least in patients with cardiac involvement, with deleterious impact on prognosis. The most known pro-thrombotic factors are heart failure, atrial fibrillation, and atrial myopathy. Atrial fibrillation could occur in 20% to 75% of systemic amyloidosis patients. Cardiac thrombi are frequently observed in patients, particularly in immunoglobulin light chains (AL) amyloidosis, up to 30%, and it is advised to look for them systematically before cardioversion. In AL amyloidosis, nephrotic syndrome and the use of immunomodulatory drugs also favour thrombosis. On the other hand, the bleeding risk increases because of frequent amyloid digestive involvement as well as factor X deficiency, renal failure, and increased risk of dysautonomia-related fall.
Keywords: Amyloidosis; Anticoagulative therapy; Bleeding; Thromboembolism.
© 2021 The Authors. ESC Heart Failure published by John Wiley & Sons Ltd on behalf of European Society of Cardiology.
Conflict of interest statement
Nothing to declare.
Figures
References
-
- Falk RH. Diagnosis and management of the cardiac amyloidoses. Circulation 2005; 112: 2047–2060. - PubMed
-
- Rapezzi C, Merlini G, Quarta CC, Riva L, Longhi S, Leone O, Salvi F, Ciliberti P, Pastorelli F, Biagini E, Coccolo F, Cooke RMT, Bacchi‐Reggiani L, Sangiorgi D, Ferlini A, Cavo M, Zamagni E, Fonte ML, Palladini G, Salinaro F, Musca F, Obici L, Branzi A, Perlini S. Systemic cardiac amyloidoses: disease profiles and clinical courses of the 3 main types. Circulation 2009; 120: 1203–1212. - PubMed
-
- Gertz MA, Dispenzieri A. Systemic amyloidosis recognition, prognosis, and therapy: a systematic review. JAMA 2020. 07; 324: 79–89. - PubMed
-
- González‐López E, Gallego‐Delgado M, Guzzo‐Merello G, de Haro‐Del Moral FJ, Cobo‐Marcos M, Robles C, Bornstein B, Salas C, Lara‐Pezzi E, Alonso‐Pulpon L, Garcia‐Pavia P. Wild‐type transthyretin amyloidosis as a cause of heart failure with preserved ejection fraction. Eur Heart J 2015; 36: 2585–2594. - PubMed
-
- Damy T, Costes B, Hagège AA, Donal E, Eicher J‐C, Slama M, Guellich A, Rappeneau S, Gueffet JP, Logeart D, Planté‐Bordeneuve V. Prevalence and clinical phenotype of hereditary transthyretin amyloid cardiomyopathy in patients with increased left ventricular wall thickness. Eur Heart J 2016. 14; 37: 1826–1834. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
