

Two-Level Anterior Cervical Discectomy and Fusion versus Hybrid Total Disc Replacement for Bilevel Pathology with Cervical Radiculopathy/Myelopathy: A Comparative Study with a Minimum 2-Year Follow-up in an Indian Population
- PMID: 34784703
- PMCID: PMC9441440
- DOI: 10.31616/asj.2021.0209
Two-Level Anterior Cervical Discectomy and Fusion versus Hybrid Total Disc Replacement for Bilevel Pathology with Cervical Radiculopathy/Myelopathy: A Comparative Study with a Minimum 2-Year Follow-up in an Indian Population
Abstract
Study design: Retrospective study.
Purpose: To study the outcomes of two-level anterior cervical discectomy and fusion (2L-ACDF) versus hybrid total disc replacement (H-TDR) for cervical myeloradiculopathy.
Overview of literature: For bilevel disc issues of the cervical spine, 2L-ACDF has been a historical tool with numerous implants used at different time frames. Recent developments in total disc replacement at mobile level with fusion at a spondylotic level known as hybrid fixation have added a new armamentarium for such disorders.
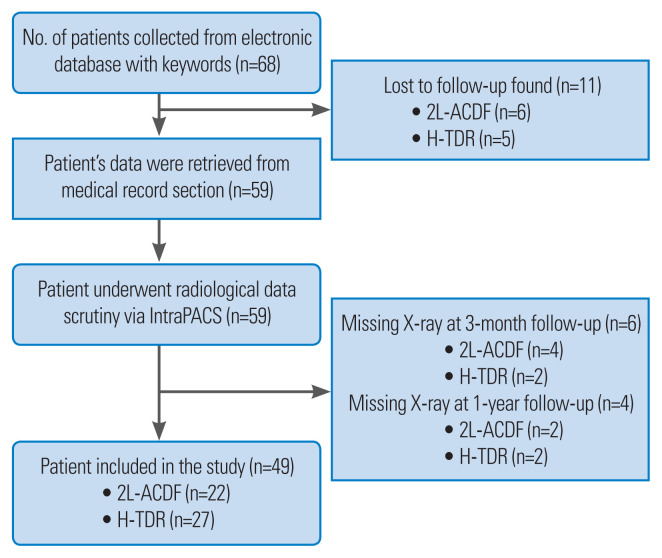
Methods: An analysis of 49 consecutive patients who underwent 2L-ACDF (n=22) and H-TDR (n=27) from January 1, 2014 to December 31, 2017 was performed. Data were studied as retrieved from InstaPACS ver. 4.0 (Mediff Technologies Pvt. Ltd., Bengaluru, India) and medical records.
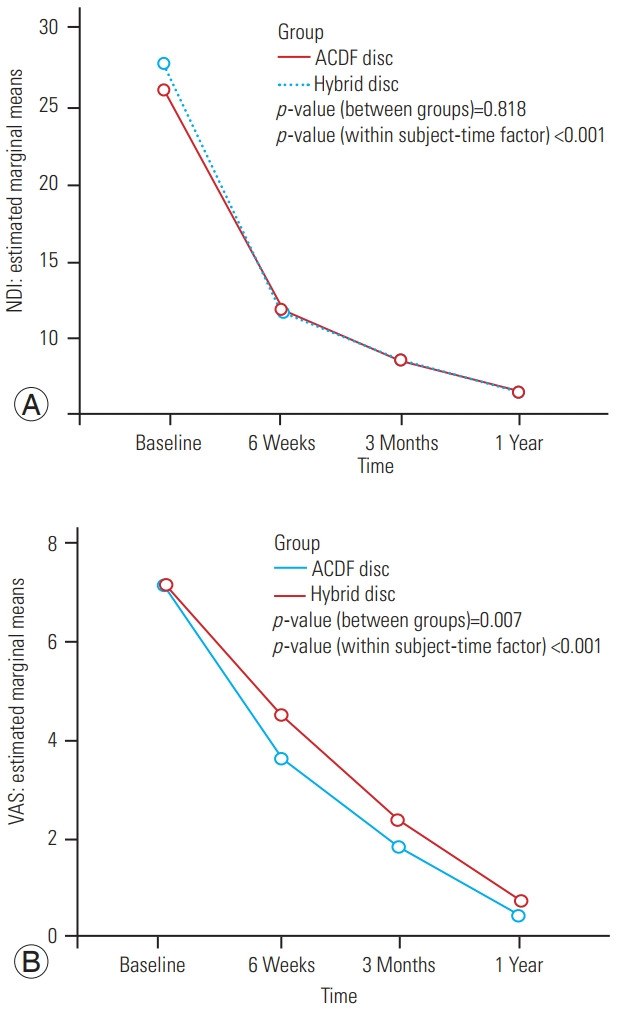
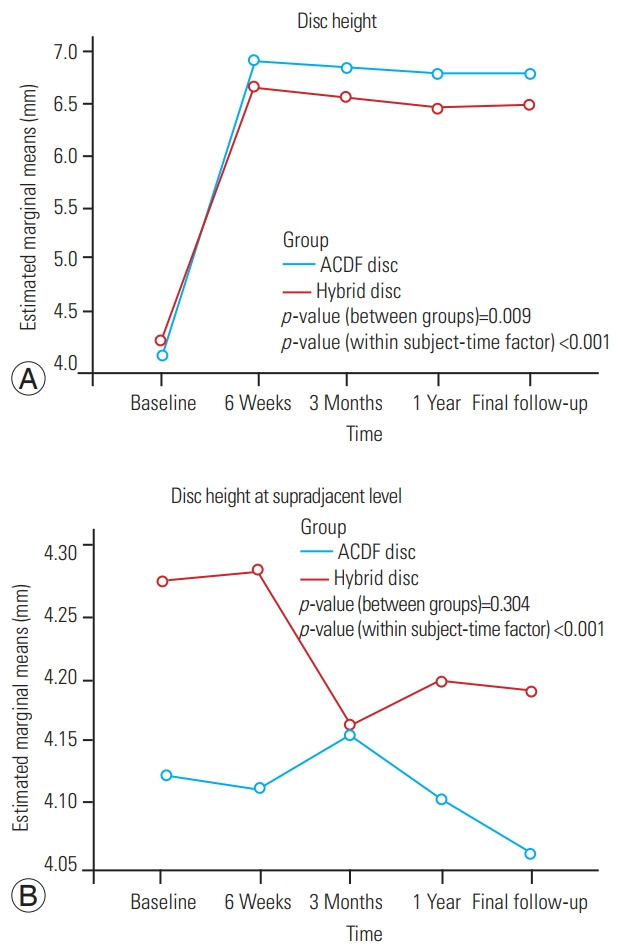
Results: Twenty-two patients with 2L-ACDF and 27 patients with H-TDR were included. The mean±standard deviation (SD) follow-up duration was 4.0±1.5 years in H-TDR and 3.1±1.1 years in 2L-ACDF. The mean±SD Neck Disability Index (NDI) decreased from 26.1±7.6 to 6.5±3.9 in the H-TDR group and from 27.6±7.2 to 6.4±4.8 in the 2L-ACDF group at final follow-up. Disc height at suprajacent level in the 2L-ACDF group was 4.12±0.48 mm, 4.10±0.45 mm, and 4.05±0.48 mm preoperatively, at 1-year, and final follow-up, respectively. Disc height at supradjacent level in the H-TDR group was 4.28±0.36 mm, 4.20±0.32 mm, and 4.19±0.34 mm preoperatively, at 1-year, and final follow-up, respectively.
Conclusions: There was significantly improved NDI in both groups. Adjacent segment disc height loss was greater in the 2L-ACDF group than in H-TDR but not statistically significant (p =0.304). Supradjacent segment range of motion was greater in the 2L-ACDF group than in the H-TDR group (p =0.003). Both findings supported radiographic adjacent segment degeneration (ASD), but symptomatic ASD was absent in both groups.
Keywords: Cervical radiculopathy; Hybrid total disc replacement; Myelopathy; Two level anterior cervical discectomy and fusion.
Conflict of interest statement
No potential conflict of interest relevant to this article was reported.
Figures
Similar articles
-
Prospective, randomized multicenter study of cervical arthroplasty versus anterior cervical discectomy and fusion: 5-year results with a metal-on-metal artificial disc.J Neurosurg Spine. 2018 Mar;28(3):252-261. doi: 10.3171/2017.5.SPINE16824. Epub 2018 Jan 5. J Neurosurg Spine. 2018. PMID: 29303467 Clinical Trial.
-
Prospective randomized study of cervical arthroplasty and anterior cervical discectomy and fusion with long-term follow-up: results in 74 patients from a single site.J Neurosurg Spine. 2013 Jan;18(1):36-42. doi: 10.3171/2012.9.SPINE12555. Epub 2012 Nov 9. J Neurosurg Spine. 2013. PMID: 23140129 Clinical Trial.
-
A Retrospective Comparative Study of Long-Term Outcomes Following Cervical Total Disc Replacement Versus Anterior Cervical Discectomy and Fusion.Cureus. 2022 Dec 11;14(12):e32399. doi: 10.7759/cureus.32399. eCollection 2022 Dec. Cureus. 2022. PMID: 36636537 Free PMC article.
-
Cervical disc arthroplasty (CDA)/total disc replacement (TDR) vs. anterior cervical diskectomy/fusion (ACDF): A review.Surg Neurol Int. 2022 Dec 2;13:565. doi: 10.25259/SNI_1028_2022. eCollection 2022. Surg Neurol Int. 2022. PMID: 36600752 Free PMC article. Review.
-
Anterior cervical discectomy and fusion (ACDF) versus cervical disc arthroplasty (CDA) for two contiguous levels cervical disc degenerative disease: a meta-analysis of randomized controlled trials.Eur Spine J. 2017 Apr;26(4):985-997. doi: 10.1007/s00586-016-4655-5. Epub 2016 Jun 17. Eur Spine J. 2017. PMID: 27314663 Review.
Cited by
-
Meta-Analysis of Treatment for Adjacent Two-Segment Cervical Spondylotic Myelopathy: A Comparison Between Anterior Cervical Corpectomy and Fusion and Anterior Cervical Discectomy and Fusion.Global Spine J. 2025 Apr;15(3):1839-1848. doi: 10.1177/21925682241297586. Epub 2024 Oct 30. Global Spine J. 2025. PMID: 39475621 Free PMC article. Review.
-
Cervical Radiculopathy: Focus on Factors for Better Surgical Outcomes and Operative Techniques.Asian Spine J. 2022 Dec;16(6):995-1012. doi: 10.31616/asj.2022.0445. Epub 2022 Dec 29. Asian Spine J. 2022. PMID: 36599372 Free PMC article.
-
Comparison of cervical disc arthroplasty versus anterior cervical discectomy and fusion for the treatment of single-segment cervical degenerative disc disease with a minimum of 4-year follow-up: a systematic review and meta-analysis of randomized controlled trials.J Orthop Surg Res. 2025 Aug 12;20(1):758. doi: 10.1186/s13018-025-06189-x. J Orthop Surg Res. 2025. PMID: 40797275 Free PMC article.
-
Clinical efficacy and complications of 10 surgical interventions for cervical ossification of the posterior longitudinal ligament: an updated systematic review and network meta-analysis.J Orthop Surg Res. 2025 Jun 7;20(1):576. doi: 10.1186/s13018-025-05878-x. J Orthop Surg Res. 2025. PMID: 40483495 Free PMC article.
-
Cervical Disc Arthroplasty (CDA) versus Anterior Cervical Discectomy and Fusion (ACDF) for Two-Level Cervical Disc Degenerative Disease: An Updated Systematic Review and Meta-Analysis.J Clin Med. 2024 May 29;13(11):3203. doi: 10.3390/jcm13113203. J Clin Med. 2024. PMID: 38892914 Free PMC article. Review.
References
-
- Gologorsky Y. Anterior cervical total disk replacement versus fusion. World Neurosurg. 2018;111:391–2. - PubMed
-
- Bohlman HH, Emery SE, Goodfellow DB, Jones PK. Robinson anterior cervical discectomy and arthrodesis for cervical radiculopathy: long-term follow-up of one hundred and twenty-two patients. J Bone Joint Surg Am. 1993;75:1298–307. - PubMed
-
- Hilibrand AS, Carlson GD, Palumbo MA, Jones PK, Bohlman HH. Radiculopathy and myelopathy at segments adjacent to the site of a previous anterior cervical arthrodesis. J Bone Joint Surg Am. 1999;81:519–28. - PubMed
-
- Barbagallo GM, Assietti R, Corbino L, et al. Early results and review of the literature of a novel hybrid surgical technique combining cervical arthrodesis and disc arthroplasty for treating multilevel degenerative disc disease: opposite or complementary techniques? Eur Spine J. 2009;18(Suppl 1):29–39. - PMC - PubMed
-
- Sekhon LH. Two-level artificial disc placement for spondylotic cervical myelopathy. J Clin Neurosci. 2004;11:412–5. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
