

Is the KDIGO Systolic Blood Pressure Target <120 mm Hg for Chronic Kidney Disease Appropriate in Routine Clinical Practice?
- PMID: 34784720
- PMCID: PMC8654101
- DOI: 10.1161/HYPERTENSIONAHA.121.18434
Is the KDIGO Systolic Blood Pressure Target <120 mm Hg for Chronic Kidney Disease Appropriate in Routine Clinical Practice?
Abstract
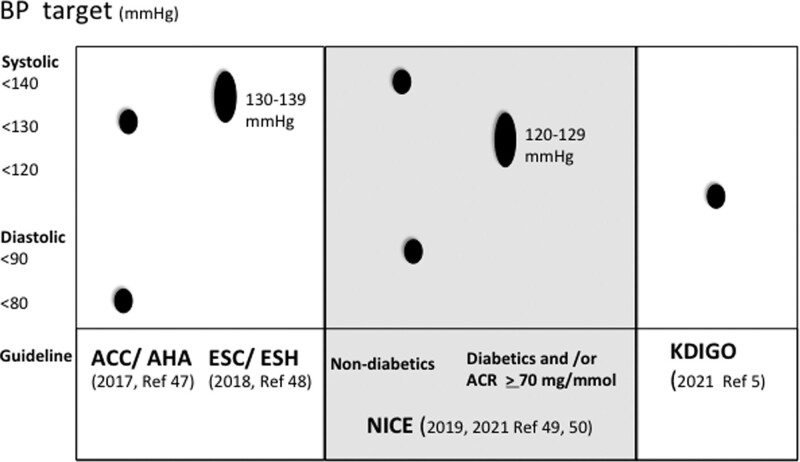
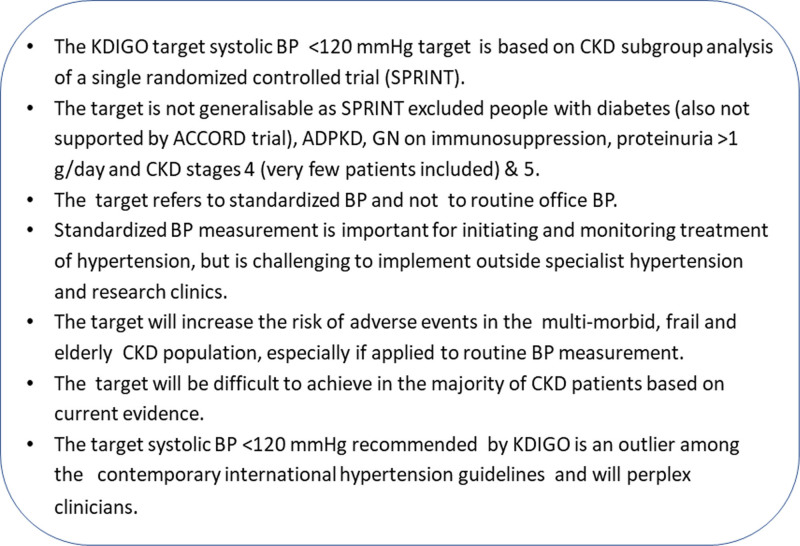
Meticulous management of hypertension is important in chronic kidney disease (CKD) to reduce the risk of cardiovascular disease, mortality, and progression of CKD. The recently published Kidney Disease Improving Global Outcomes (KDIGO) guideline on blood pressure (BP) management in CKD stresses the importance of standardized BP measurement and strict control of BP. This is a useful document that will help to improve the management of hypertension in CKD globally. However, the recommendation of systolic BP target of <120 mm Hg by KDIGO is controversial. It is based on weak evidence derived mainly from a single randomized controlled trial and its CKD subgroup analysis. Here, we review the current evidence surrounding BP target in CKD. We argue that the target recommended by KDIGO is not generalizable to the majority of people with CKD. Standardized BP measurements are challenging to implement outside specialist hypertension and research clinics, and the target of <120 mm Hg BP systolic cannot be extrapolated to routine clinic BP measurements. If applied to routine BP measurement, this target will expose the multimorbid and frail CKD patients to the risk of adverse events including falls and fractures. Furthermore, it will not be achievable in the majority of CKD patients. The target recommended by KDIGO is an outlier among contemporary major international hypertension guidelines and is likely to perplex clinicians. We believe the KDIGO-recommended target systolic BP <120 mm Hg for CKD is inappropriate in the majority of CKD patients and it may even be harmful for patients managed in routine clinical practice.
Keywords: accidental falls; blood pressure; frail elderly; guideline; hypertension.
Figures
References
-
- Roth GA, Mensah GA, Johnson CO, Addolorato G, Ammirati E, Baddour LM, Barengo NC, Beaton AZ, Benjamin EJ, Benziger CP, et al. ; GBD-NHLBI-JACC Global Burden of Cardiovascular Diseases Writing Group. Global burden of cardiovascular diseases and risk factors, 1990-2019: update from the GBD 2019 study. J Am Coll Cardiol. 2020;76:2982–3021. doi: 10.1016/j.jacc.2020.11.010 - PMC - PubMed
-
- Sarnak MJ, Greene T, Wang X, Beck G, Kusek JW, Collins AJ, Levey AS. The effect of a lower target blood pressure on the progression of kidney disease: long-term follow-up of the modification of diet in renal disease study. Ann Intern Med. 2005;142:342–351. doi: 10.7326/0003-4819-142-5-200503010-00009 - PubMed
-
- Keith DS, Nichols GA, Gullion CM, Brown JB, Smith DH. Longitudinal follow-up and outcomes among a population with chronic kidney disease in a large managed care organization. Arch Intern Med. 2004;164:659–663. doi: 10.1001/archinte.164.6.659 - PubMed
-
- Go AS, Chertow GM, Fan D, McCulloch CE, Hsu CY. Chronic kidney disease and the risks of death, cardiovascular events, and hospitalization. N Engl J Med. 2004;351:1296–1305. doi: 10.1056/NEJMoa041031 - PubMed
-
- Cheung AK, Chang TI, Cushman WC, Furth SL, Hou FF, Ix JH, Knoll GA, Muntner P, Pecoits-Filho R, Sarnak MJ, et al. . Executive summary of the KDIGO 2021 clinical practice guideline for the management of blood pressure in chronic kidney disease. Kidney Int. 2021;99:559–569. doi: 10.1016/j.kint.2020.10.026 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
