

Comparison of the analgesic effect of ultrasound-guided paravertebral block and ultrasound-guided retrolaminar block in Uniportal video-assisted Thoracoscopic surgery: a prospective, randomized study
- PMID: 34784889
- PMCID: PMC8594110
- DOI: 10.1186/s12885-021-08938-7
Comparison of the analgesic effect of ultrasound-guided paravertebral block and ultrasound-guided retrolaminar block in Uniportal video-assisted Thoracoscopic surgery: a prospective, randomized study
Abstract
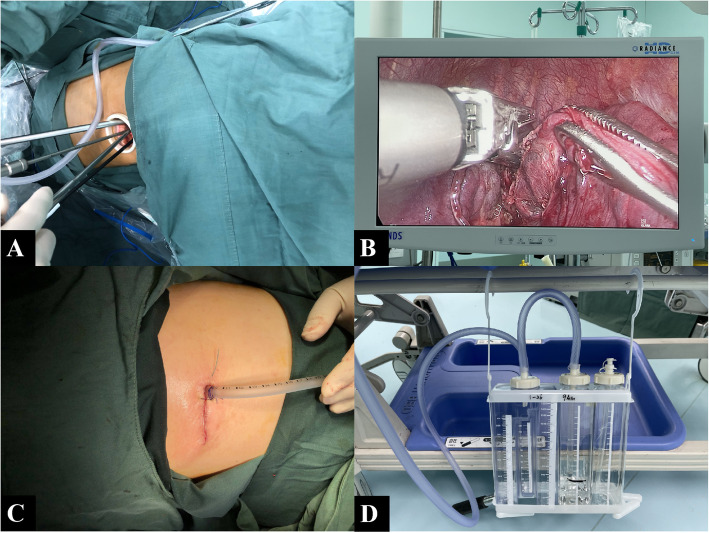
Background: The optimal modality for postoperative analgesia after uniportal video-assisted thoracoscopic surgery (UVATS) for the treatment of lung cancer has not yet been determined. Both ultrasound-guided paravertebral block (PVB) and retrolaminar block (RLB) have been reported to be successful in providing analgesia after UVATS. However, which block technique provides superior analgesia after UVATS is still unclear. This randomized study was designed to compare the postoperative analgesic effects and adverse events associated with ultrasound-guided PVB and RLB after UVATS.
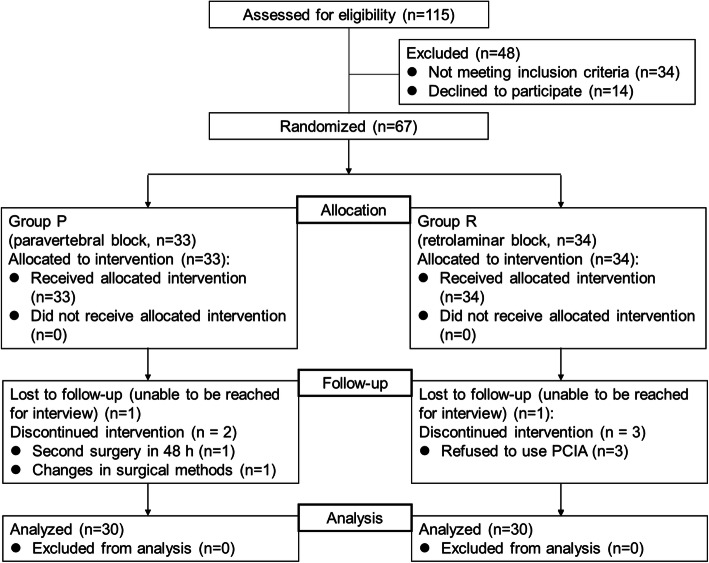
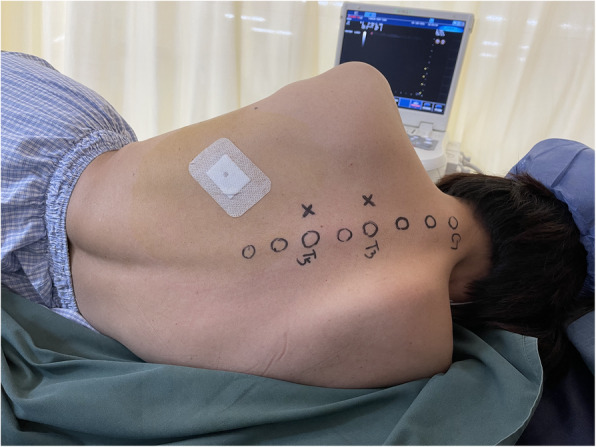
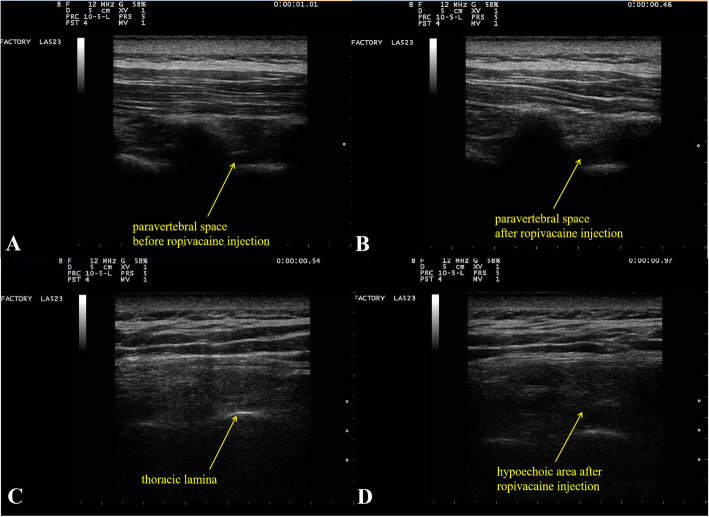
Methods: Sixty patients with lung cancer were randomized to undergo ultrasound-guided PVB (group P) or ultrasound-guided RLB (group R). In group P, 30 mL of 0.5% ropivacaine was injected at the T3 and T5 levels via ultrasound-guided PVB (15 mL at each level on the operative side). In group R, 30 mL of 0.5% ropivacaine was injected at the T3 and T5 levels via ultrasound-guided RLB (15 mL at each level on the operative side). The primary outcome was the numerical rating scale (NRS) score within 48 h after surgery. The secondary outcomes were total postoperative sufentanil consumption, time to first analgesic request and adverse events.
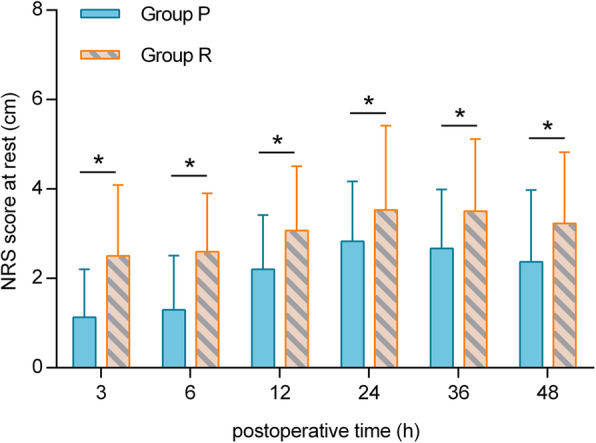
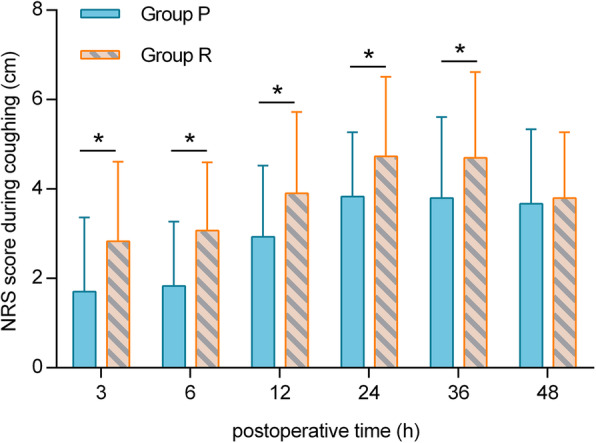
Results: At 3, 6, 12, 24, 36 and 48 h postoperatively, the NRS score at rest in group P was lower than that in group R (p < 0.05). At 3, 6, 12, 24 and 36 h postoperatively, the NRS score while coughing in group P was lower than that in group R (p < 0.05). The total postoperative sufentanil consumption in group P was significantly lower than that in group R (p < 0.001). Additionally, the time to first analgesic request was longer in group R than in group P (p < 0.0001). The incidence of nausea in group R was higher than that in group P (p < 0.05).
Conclusions: In patients with lung cancer undergoing UVATS, ultrasound-guided PVB with 0.5% ropivacaine provides better analgesia and results in less nausea than ultrasound-guided RLB. Compared with ultrasound-guided RLB, ultrasound-guided PVB seems to be a better technique for analgesia in UVATS.
Trial registration: The name of this study is the Effect And Mechanism Of Ultrasound-guided Multimodal Regional Nerve Block On Acute And Chronic Pain After Thoracic Surgery. This study was registered in the Chinese Clinical Trial Registry ( ChiCTR2100044060 ). The date of registration was March 9, 2021.
Keywords: Adverse events; Lung cancer; Pain; Ultrasound-guided paravertebral block; Ultrasound-guided retrolaminar block; Uniportal video-assisted thoracoscopic surgery.
© 2021. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Similar articles
-
Comparison of different adjuvant analgesia for paravertebral block in video-assisted thoracoscopic surgery: A double-blind randomized controlled trial.PLoS One. 2025 May 2;20(5):e0322589. doi: 10.1371/journal.pone.0322589. eCollection 2025. PLoS One. 2025. PMID: 40315237 Free PMC article. Clinical Trial.
-
Comparison Between Intraoperative Two-Space Injection Thoracic Paravertebral Block and Wound Infiltration as a Component of Multimodal Analgesia for Postoperative Pain Management After Video-Assisted Thoracoscopic Lobectomy: A Randomized Controlled Trial.J Cardiothorac Vasc Anesth. 2015 Dec;29(6):1550-6. doi: 10.1053/j.jvca.2015.06.013. Epub 2015 Jun 10. J Cardiothorac Vasc Anesth. 2015. PMID: 26409920 Clinical Trial.
-
Adding sufentanil to ropivacaine in continuous thoracic paravertebral block fails to improve analgesia after video-assisted thoracic surgery: A randomised controlled trial.Eur J Anaesthesiol. 2018 Oct;35(10):766-773. doi: 10.1097/EJA.0000000000000777. Eur J Anaesthesiol. 2018. PMID: 29373333 Clinical Trial.
-
A comparison of regional anesthesia techniques in patients undergoing video-assisted thoracic surgery: A network meta-analysis.Int J Surg. 2022 Sep;105:106840. doi: 10.1016/j.ijsu.2022.106840. Epub 2022 Aug 24. Int J Surg. 2022. PMID: 36030040 Review.
-
Epidural analgesia versus paravertebral block in video-assisted thoracoscopic surgery.Interact Cardiovasc Thorac Surg. 2019 Mar 1;28(3):404-406. doi: 10.1093/icvts/ivy265. Interact Cardiovasc Thorac Surg. 2019. PMID: 30169855 Review.
Cited by
-
Anatomical classification and clinical application of thoracic paraspinal blocks.Korean J Anesthesiol. 2022 Aug;75(4):295-306. doi: 10.4097/kja.22138. Epub 2022 Apr 4. Korean J Anesthesiol. 2022. PMID: 35368174 Free PMC article.
-
The effect of preemptive retrolaminar block on lumbar spinal decompression surgery.Eur Spine J. 2024 Nov;33(11):4253-4261. doi: 10.1007/s00586-024-08219-4. Epub 2024 Jun 17. Eur Spine J. 2024. PMID: 38886235
-
Comparison of thoracoscopy-guided thoracic paravertebral block and patient-controlled intravenous analgesia for postoperative analgesia after uniportal thoracoscopic pulmonary wedge resection: a prospective randomized controlled trial.Front Med (Lausanne). 2025 May 15;12:1554515. doi: 10.3389/fmed.2025.1554515. eCollection 2025. Front Med (Lausanne). 2025. PMID: 40443516 Free PMC article.
-
The effect of ultrasound-guided bilateral thoracic retrolaminar block on analgesia after pediatric open cardiac surgery: a randomized controlled double-blind study.Korean J Anesthesiol. 2022 Jun;75(3):276-282. doi: 10.4097/kja.21466. Epub 2022 Jan 12. Korean J Anesthesiol. 2022. PMID: 35016497 Free PMC article. Clinical Trial.
-
Effect of Dinalbuphine sebacate on postoperative multimodal analgesic strategy in video-assisted thoracoscopic surgery: a double-blind randomized controlled trial.BMC Anesthesiol. 2025 May 17;25(1):252. doi: 10.1186/s12871-025-03118-7. BMC Anesthesiol. 2025. PMID: 40382572 Free PMC article. Clinical Trial.
References
-
- Sihoe ADL. Video-assisted thoracoscopic surgery as the gold standard for lung cancer surgery. Respirology. 2020;(Suppl 2):49–60. 10.1111/resp.13920. - PubMed
-
- Elsabeeny WY, Ibrahim MA, Shehab NN, Mohamed A, Wadod MA. Serratus anterior plane block and erector spinae plane block versus thoracic epidural analgesia for perioperative thoracotomy pain control: a randomized controlled study. J Cardiothorac Vasc Anesth. 2021;35(10):2928–2936. doi: 10.1053/j.jvca.2020.12.047. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
