

Reduction of cardiovascular risk factors among young men with hypertension using an interactive decision aid: cluster-randomized control trial
- PMID: 34784891
- PMCID: PMC8596802
- DOI: 10.1186/s12872-021-02339-1
Reduction of cardiovascular risk factors among young men with hypertension using an interactive decision aid: cluster-randomized control trial
Abstract
Background: Coronary heart disease (CHD) mortality among young men is very high and the prevention methods usable in family practice (FP) settings are limited (1,2). The objectives of this study were to investigate the cardiovascular risk profile among young males (18-50) visiting their family doctor (FD) and to find out if using an interactive computer-based decision aid (DA) has advantages in reducing cardiovascular risk factors compared to usual counselling at the FD's office.
Methods: The study was a cluster-randomized controlled trial including hypertensive male patients aged 18-50 recruited by their FD in 2015-2016. Patients with cardiovascular complications were not included. FDs were randomly divided into intervention groups (n = 9) and control groups (n = 11). Altogether, FDs recruited 130 patients, 77 into the intervention group (IG) and 53 into the control group (CG). IG patients were counselled about cardiovascular risk factors using a computer-based DA. CG patients received usual counselling by their FD. Data was collected with questionnaires, clinical examinations and laboratory analyses at the baseline and at the follow-up visit three months later. We compared the cardiovascular risk factors of the IG and CG patients.
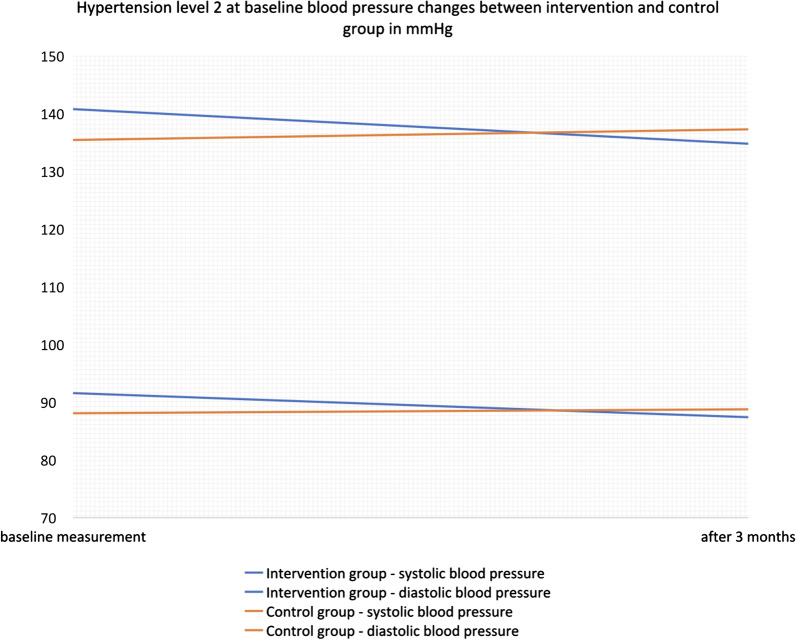
Results: Baseline characteristics of the IG and CG patients were comparable. Of the whole study group, 51.5% (n = 67) of the patients had hypertension grade 1, 45.4% (n = 59) had grade 2 and 3.1% (n = 4) had grade 3. Twenty-seven per cent (n = 21) of the IG and 42% (n = 22) of the CG patients were smokers. We found that shared decision making with the DA was more effective in smoking reduction compared to usual FD counselling: 21 smoking patients in the IG reduced the number of cigarettes per day which is significantly more than the 22 smoking patients in the CG (- 3.82 ± 1.32 (SE Mean) versus + 2.32 ± 1.29; p = 0.001). Systolic blood pressure (SBP), diastolic blood pressure (DBP) and the number of cigarettes per day, all showed a statistically significant reduction among patients who were using the DA. Male patients with hypertension grade 2 had a significantly greater reduction in their SBP (- 6.003 ± 2.59 (SE Mean) versus + 1.86 ± 2.58; p = 0.038) grade 1. Reduction of DBP, cigarettes per day and CVD risk in general were nearly significant in the IG whereas the CG showed an increase in all of these parameters.
Conclusion: Using interactive DAs at FD's offices for counselling of young hypertensive male patients is one possibility to help patients understand their risk factors and make changes in their treatment choices. DAs can be more effective in achieving behavioural changes like reducing smoking or blood pressure compared to normal counselling.
Keywords: Cardiovascular risk; Decision aid; Hypertension; Shared decision making.
© 2021. The Author(s).
Conflict of interest statement
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of this article.
Figures
References
-
- Fritz J, Edlinger M, Kelleher C, Strohmaier S, Nagel G, Concin H, et al. Mediation analysis of the relationship between sex, cardiovascular risk factors and mortality from coronary heart disease: findings from the population-based VHM&PP cohort. Atherosclerosis. 2015;243(1):86–92. doi: 10.1016/j.atherosclerosis.2015.08.048. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
