

Expansion of myeloid-derived suppressor cells contributes to metabolic osteoarthritis through subchondral bone remodeling
- PMID: 34784965
- PMCID: PMC8594239
- DOI: 10.1186/s13075-021-02663-z
Expansion of myeloid-derived suppressor cells contributes to metabolic osteoarthritis through subchondral bone remodeling
Abstract
Background: Osteoarthritis (OA) subsequent to acute joint injury accounts for a significant proportion of all arthropathies. Myeloid-derived suppressor cells (MDSCs) are a heterogeneous population of myeloid progenitor cells classically known for potent immune-suppressive activity; however, MDSCs can also differentiate into osteoclasts. In addition, this population is known to be expanded during metabolic disease. The objective of this study was to determine the role of MDSCs in the context of OA pathophysiology.
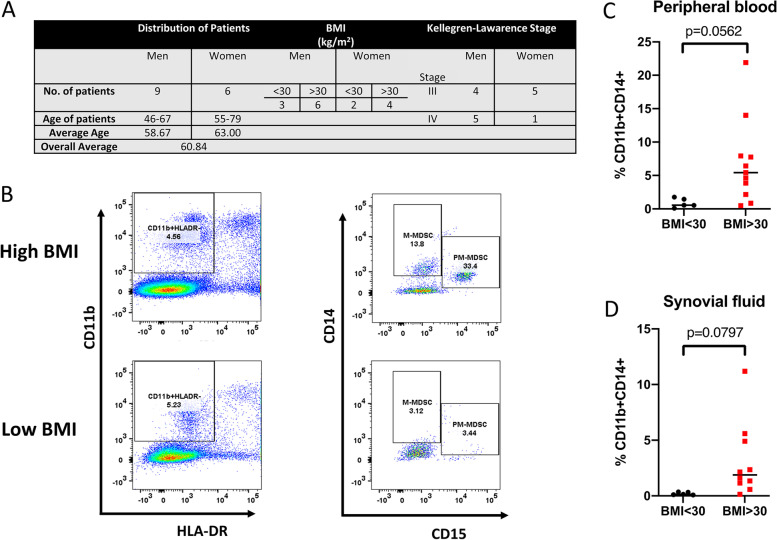
Methods: In this study, we examined the differentiation and functional capacity of MDSCs to become osteoclasts in vitro and in vivo using mouse models of OA and in MDSC quantitation in humans with OA pathology relative to obesity status.
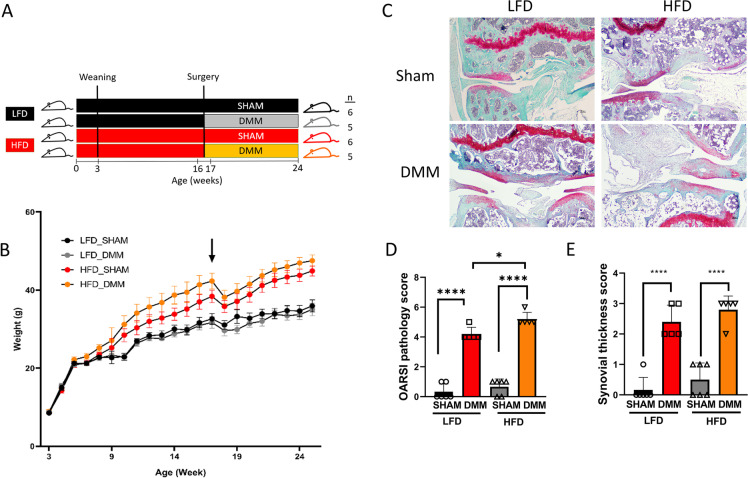
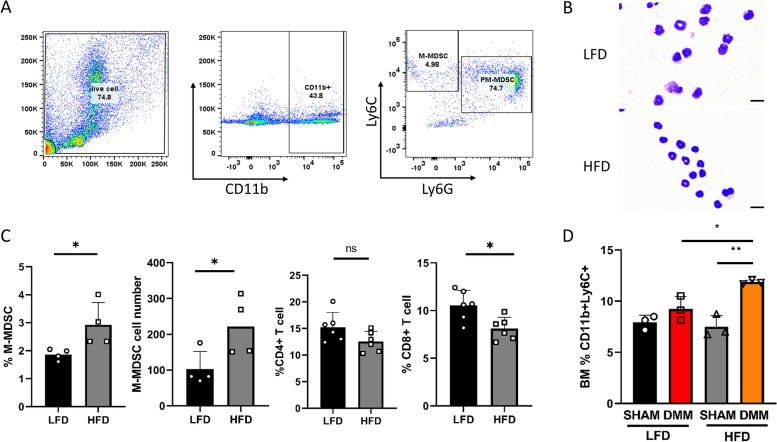
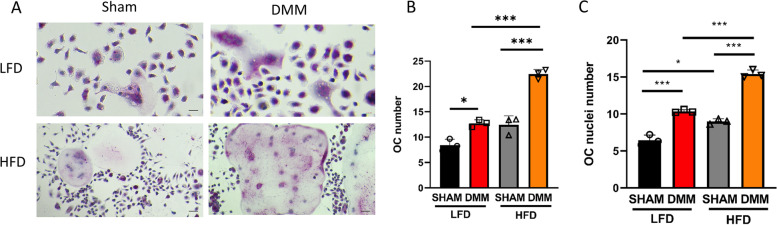
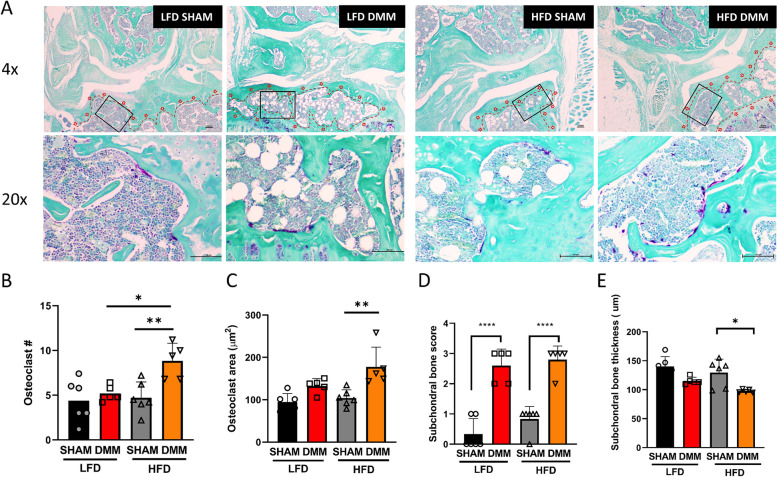
Results: We observed that MDSCs are expanded in mice and humans during obesity. MDSCs were expanded in peripheral blood of OA subjects relative to body mass index and in mice fed a high-fat diet (HFD) compared to mice fed a low-fat diet (LFD). In mice, monocytic MDSC (M-MDSC) was expanded in diet-induced obesity (DIO) with a further expansion after destabilization of the medial meniscus (DMM) surgery to induce post-traumatic OA (PTOA) (compared to sham-operated controls). M-MDSCs from DIO mice had a greater capacity to form osteoclasts in culture with increased subchondral bone osteoclast number. In humans, we observed an expansion of M-MDSCs in peripheral blood and synovial fluid of obese subjects compared to lean subjects with OA.
Conclusion: These data suggest that MDSCs are reprogrammed in metabolic disease, with the potential to contribute towards OA progression and severity.
Keywords: Myeloid-derived suppressor cells; Obesity; Osteoarthritis; Osteoclasts; Subchondral bone.
© 2021. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Felson DT, Lawrence RC, Dieppe PA, Hirsch R, Helmick CG, Jordan JM, Kington RS, Lane NE, Nevitt MC, Zhang Y, Sowers M, McAlindon T, Spector TD, Poole AR, Yanovski SZ, Ateshian G, Sharma L, Buckwalter JA, Brandt KD, Fries JF. Osteoarthritis: new insights. Part 1: the disease and its risk factors. Ann Intern Med. 2000;133(8):635–646. doi: 10.7326/0003-4819-133-8-200010170-00016. - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
