

Detecting Liquid Remnants of Solid Tumors: Circulating Tumor DNA Minimal Residual Disease
- PMID: 34785539
- PMCID: PMC8976700
- DOI: 10.1158/2159-8290.CD-21-0634
Detecting Liquid Remnants of Solid Tumors: Circulating Tumor DNA Minimal Residual Disease
Abstract
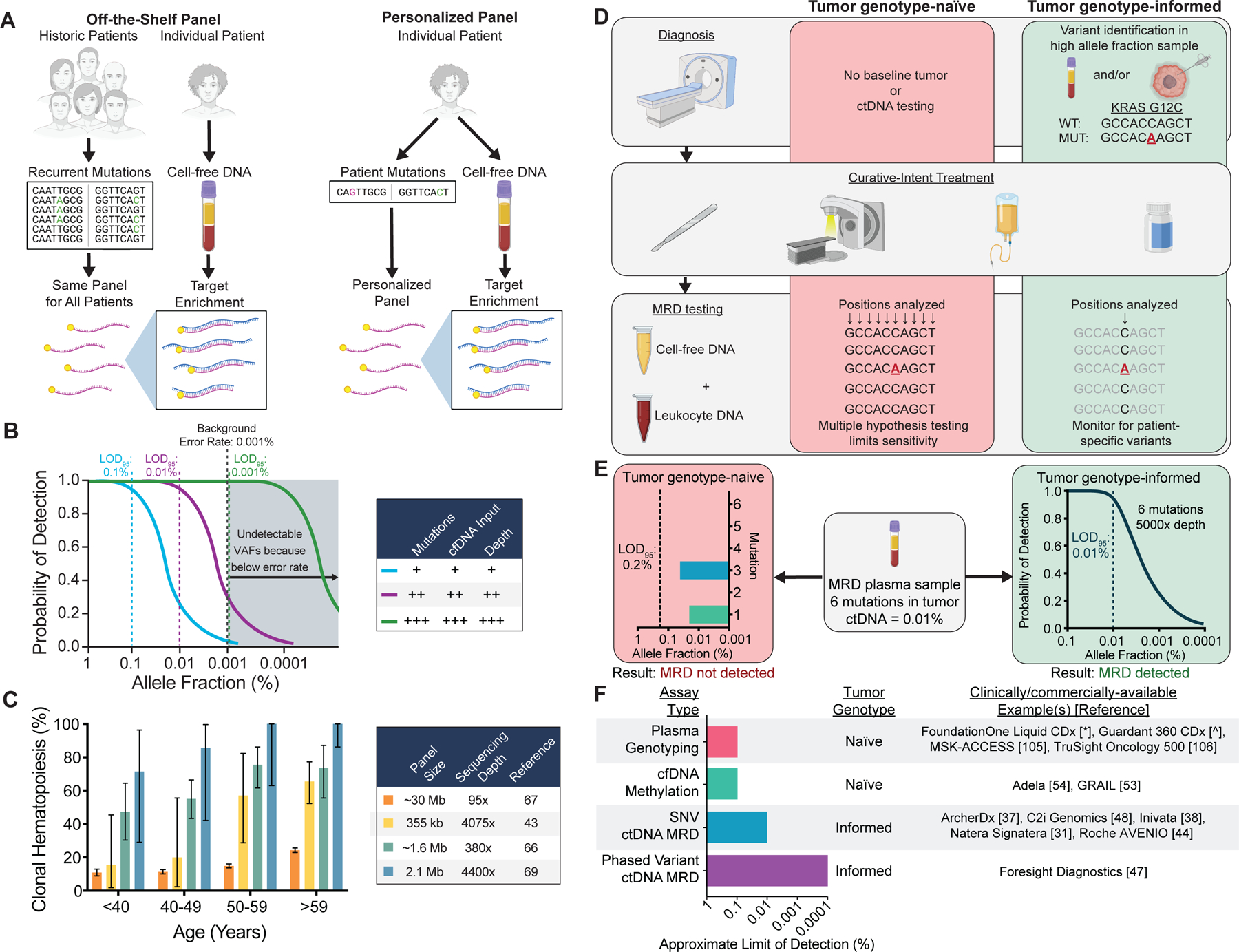
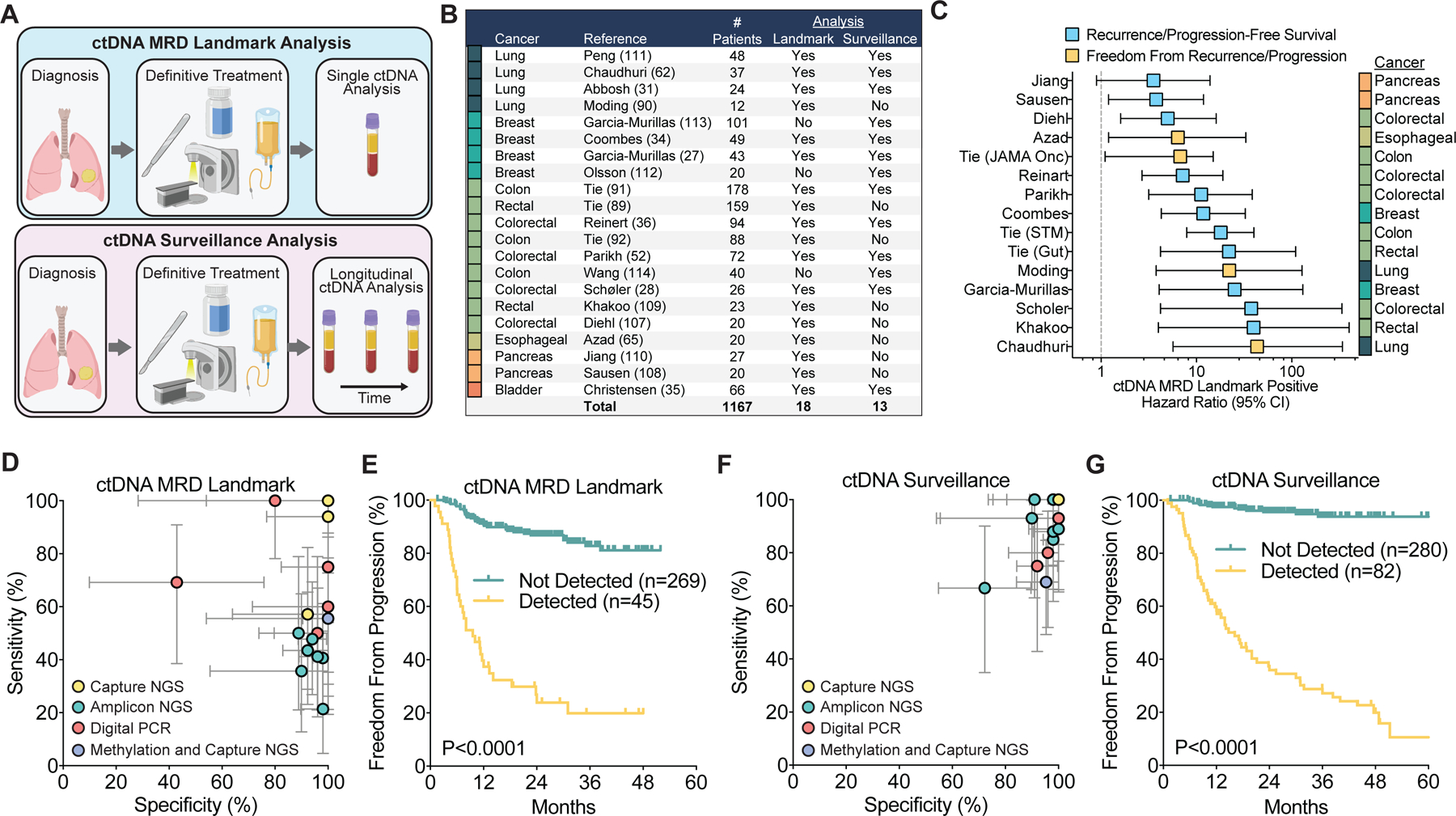
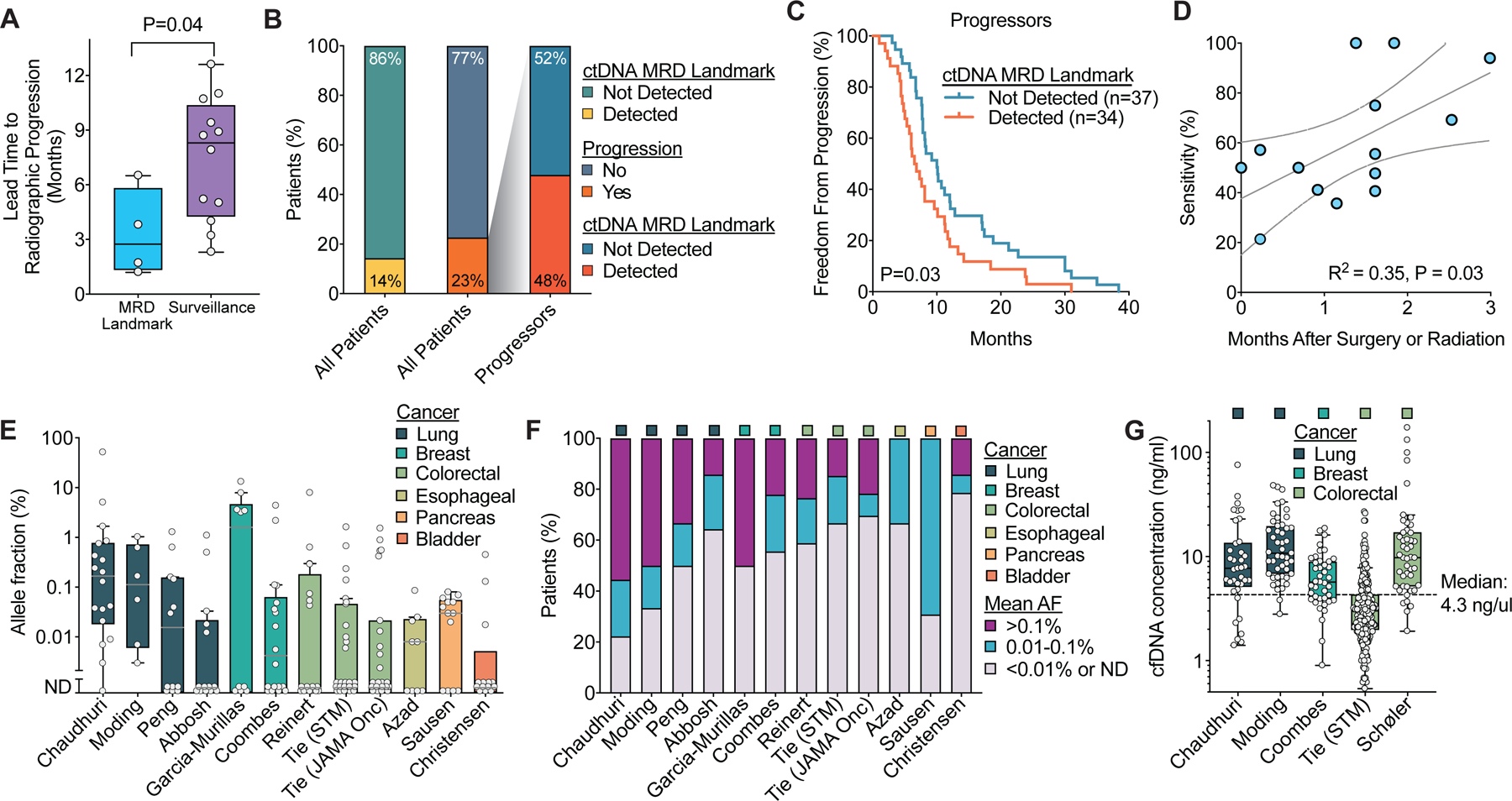
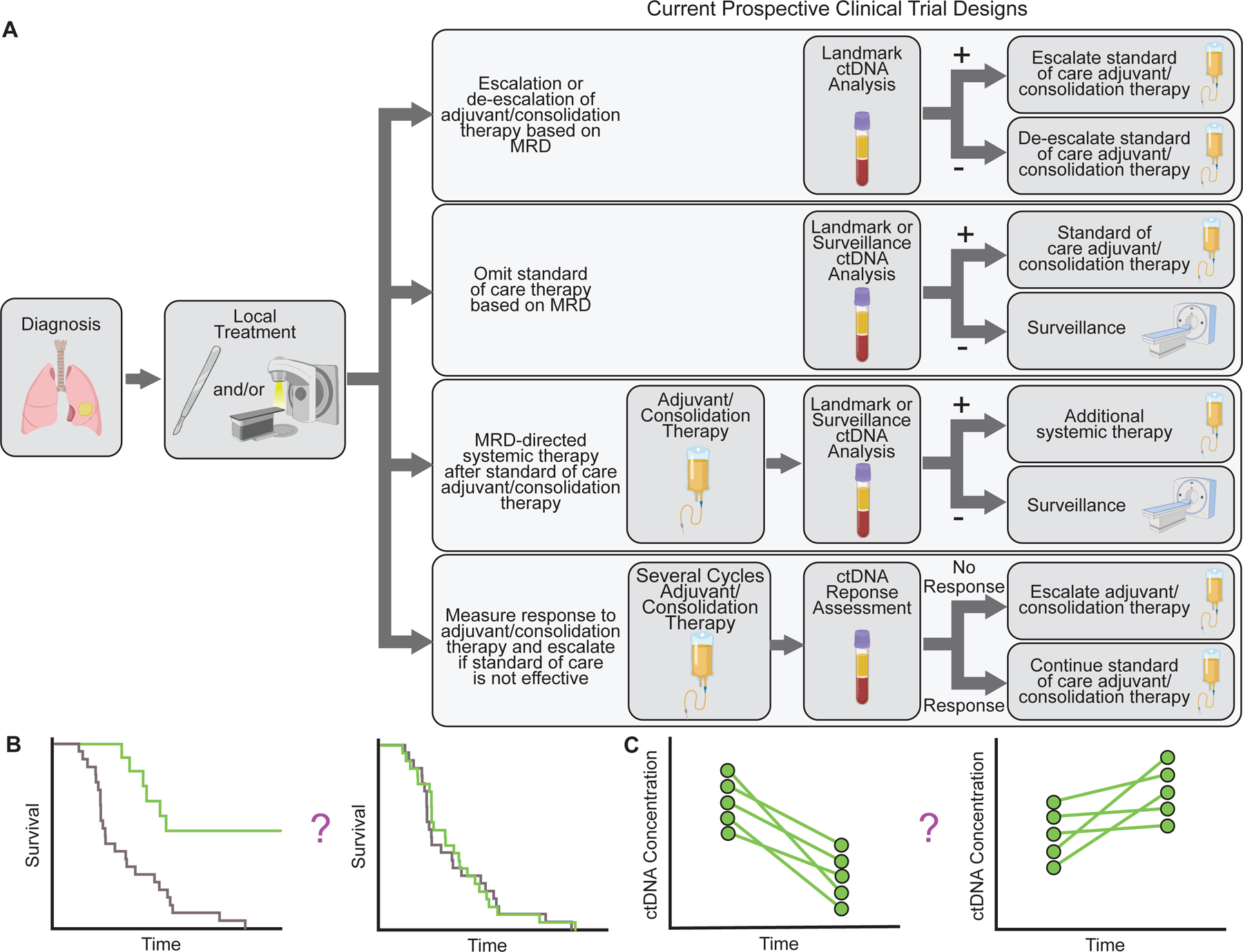
Growing evidence demonstrates that circulating tumor DNA (ctDNA) minimal residual disease (MRD) following treatment for solid tumors predicts relapse. These results suggest that ctDNA MRD could identify candidates for adjuvant therapy and measure response to such treatment. Importantly, factors such as assay type, amount of ctDNA release, and technical and biological background can affect ctDNA MRD results. Furthermore, the clinical utility of ctDNA MRD for treatment personalization remains to be fully established. Here, we review the evidence supporting the value of ctDNA MRD in solid cancers and highlight key considerations in the application of this potentially transformative biomarker.
Significance: ctDNA analysis enables detection of MRD and predicts relapse after definitive treatment for solid cancers, thereby promising to revolutionize personalization of adjuvant and consolidation therapies.
©2021 American Association for Cancer Research.
Conflict of interest statement
Competing Interests
E.J.M. has served as a paid consultant for DeciBio. B.Y.N. is currently an employee and stockholder at Roche/Genentech and has patent filings related to immunomodulatory RNA and cancer biomarkers. A.A.A. and M.D. are co-inventors on patent applications related to CAPP-Seq and have patent filings related to other cancer biomarkers. A.A.A. reports ownership interest in CiberMed and Foresight Diagnostics, paid consultancy from Roche/Genentech and Gilead, and research support from BMS. M. Diehn reports research funding from Varian Medical Systems, AstraZeneca, and Illumina, ownership interest in CiberMed and Foresight Diagnostics, patent filings related to cancer biomarkers, paid consultancy from AstraZeneca, Genentech, Novartis, Boehringer Ingelheim, Illumina, Roche Sequencing Solutions, Gritstone Oncology, and BioNTech, and travel/honoraria from RefleXion.
Figures
References
-
- Siegel RL, Miller KD, Fuchs HE, Jemal A. Cancer Statistics, 2021. CA Cancer J Clin. 2021;71:7–33. - PubMed
-
- Goddard ET, Bozic I, Riddell SR, Ghajar CM. Dormant tumour cells, their niches and the influence of immunity. Nat Cell Biol. 2018;20:1240–9. - PubMed
-
- Pignon J-P, Tribodet H, Scagliotti GV, Douillard J-Y, Shepherd FA, Stephens RJ, et al. Lung adjuvant cisplatin evaluation: a pooled analysis by the LACE Collaborative Group. J Clin Oncol. 2008;26:3552–9. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
