

Unexplained mortality during the US COVID-19 pandemic: retrospective analysis of death certificate data and critical assessment of excess death calculations
- PMID: 34785551
- PMCID: PMC8595295
- DOI: 10.1136/bmjopen-2021-050361
Unexplained mortality during the US COVID-19 pandemic: retrospective analysis of death certificate data and critical assessment of excess death calculations
Abstract
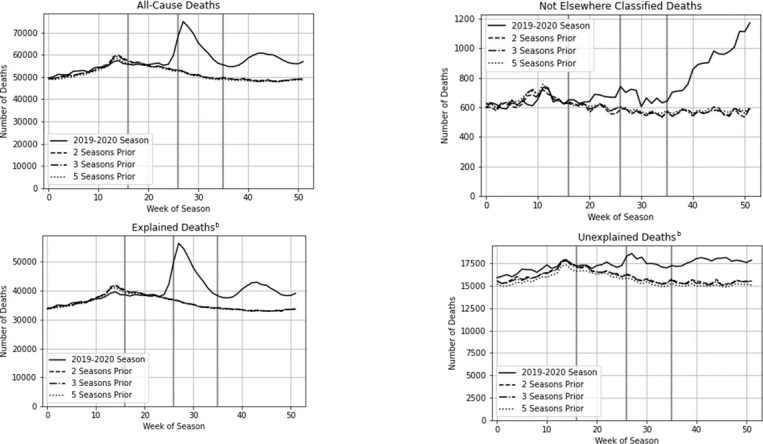
Objectives: Cause-of-death discrepancies are common in respiratory illness-related mortality. A standard epidemiological metric, excess all-cause death, is unaffected by these discrepancies but provides no actionable policy information when increased all-cause mortality is unexplained by reported specific causes. To assess the contribution of unexplained mortality to the excess death metric, we parsed excess deaths in the COVID-19 pandemic into changes in explained versus unexplained (unreported or unspecified) causes.
Design: Retrospective repeated cross-sectional analysis, US death certificate data for six influenza seasons beginning October 2014, comparing population-adjusted historical benchmarks from the previous two, three and five seasons with 2019-2020.
Setting: 48 of 50 states with complete data.
Participants: 16.3 million deaths in 312 weeks, reported in categories-all causes, top eight natural causes and respiratory causes including COVID-19.
Outcome measures: Change in population-adjusted counts of deaths from seasonal benchmarks to 2019-2020, from all causes (ie, total excess deaths) and from explained versus unexplained causes, reported for the season overall and for time periods defined a priori: pandemic awareness (19 January through 28 March); initial pandemic peak (29 March through 30 May) and pandemic post-peak (31 May through 26 September).
Results: Depending on seasonal benchmark, 287 957-306 267 excess deaths occurred through September 2020: 179 903 (58.7%-62.5%) attributed to COVID-19; 44 022-49 311 (15.2%-16.1%) to other reported causes; 64 032-77 054 (22.2%-25.2%) unexplained (unspecified or unreported cause). Unexplained deaths constituted 65.2%-72.5% of excess deaths from 19 January to 28 March and 14.1%-16.1% from 29 March through 30 May.
Conclusions: Unexplained mortality contributed substantially to US pandemic period excess deaths. Onset of unexplained mortality in February 2020 coincided with previously reported increases in psychotropic use, suggesting possible psychiatric or injurious causes. Because underlying causes of unexplained deaths may vary by group or region, results suggest excess death calculations provide limited actionable information, supporting previous calls for improved cause-of-death data to support evidence-based policy.
Keywords: COVID-19; epidemiology; health informatics; mental health; public health; statistics & research methods.
© Author(s) (or their employer(s)) 2021. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: KAF is President and JDR is Research Intern with Kathleen Fairman LTD, a for-profit research consulting firm. Kathleen Fairman LTD provided analytical support and article processing charges but has no financial or non-financial interests related to the topic of the manuscript. KJG and RSZ have no competing interests to report.
Figures
Similar articles
-
Estimation of Excess Deaths Associated With the COVID-19 Pandemic in the United States, March to May 2020.JAMA Intern Med. 2020 Oct 1;180(10):1336-1344. doi: 10.1001/jamainternmed.2020.3391. JAMA Intern Med. 2020. PMID: 32609310 Free PMC article.
-
COVID-19 pandemic: Coroner's database of death inquiries with clinical epidemiology and total and excess mortality analyses in the District of Kildare March to June 2020.J Forensic Leg Med. 2020 Nov;76:102072. doi: 10.1016/j.jflm.2020.102072. Epub 2020 Oct 31. J Forensic Leg Med. 2020. PMID: 33157341 Free PMC article.
-
Disentangling the relationship between cancer mortality and COVID-19 in the US.Elife. 2024 Aug 27;13:RP93758. doi: 10.7554/eLife.93758. Elife. 2024. PMID: 39190600 Free PMC article.
-
Every Body Counts: Measuring Mortality From the COVID-19 Pandemic.Ann Intern Med. 2020 Dec 15;173(12):1004-1007. doi: 10.7326/M20-3100. Epub 2020 Sep 11. Ann Intern Med. 2020. PMID: 32915654 Free PMC article. Review.
-
Flaws and uncertainties in pandemic global excess death calculations.Eur J Clin Invest. 2023 Aug;53(8):e14008. doi: 10.1111/eci.14008. Epub 2023 Apr 24. Eur J Clin Invest. 2023. PMID: 37067255 Free PMC article. Review.
Cited by
-
Excess non-COVID-19 mortality in Norway 2020-2022.BMC Public Health. 2024 Jan 22;24(1):244. doi: 10.1186/s12889-023-17515-5. BMC Public Health. 2024. PMID: 38254068 Free PMC article.
-
Excess mortality from COVID 19 in Costa Rica: a registry based study using Poisson regression.Lancet Reg Health Am. 2023 Apr;20:100451. doi: 10.1016/j.lana.2023.100451. Epub 2023 Feb 22. Lancet Reg Health Am. 2023. PMID: 36852399 Free PMC article.
-
Using an online calculator to describe excess mortality in the Philippines during the COVID-19 pandemic.Western Pac Surveill Response J. 2023 Mar 22;14(1):1-11. doi: 10.5365/wpsar.2023.14.1.984. eCollection 2023 Jan-Mar. Western Pac Surveill Response J. 2023. PMID: 37064545 Free PMC article.
References
-
- U.S. Centers for Disease Control and Prevention . People at increased risk for severe illness: older adults, people with medical conditions, 2021. Available: https://www.cdc.gov/coronavirus/2019-ncov/need-extra-precautions/index.html
MeSH terms
LinkOut - more resources
Full Text Sources
Medical