

Bosentan combined with sildenafil in the treatment of COPD patients with pulmonary arterial hypertension
- PMID: 34786078
- PMCID: PMC8581888
Bosentan combined with sildenafil in the treatment of COPD patients with pulmonary arterial hypertension
Abstract
Objective: To explore the impacts of bosentan combined with sildenafil on chronic obstructive pulmonary disease (COPD) patients with pulmonary arterial hypertension (PAH).
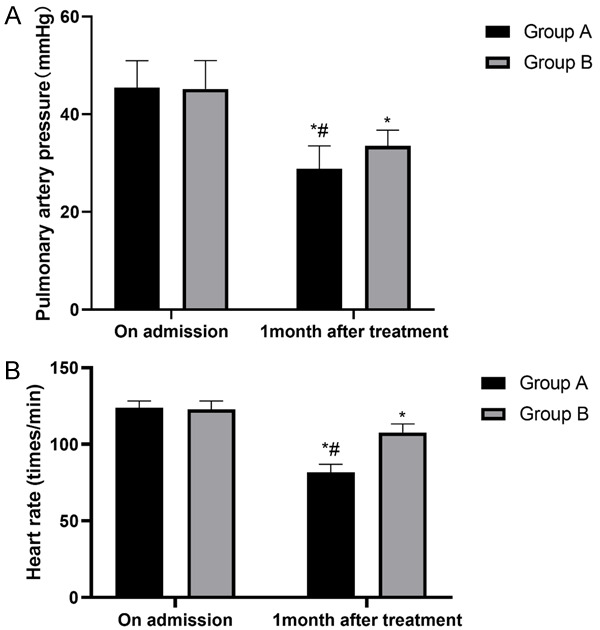
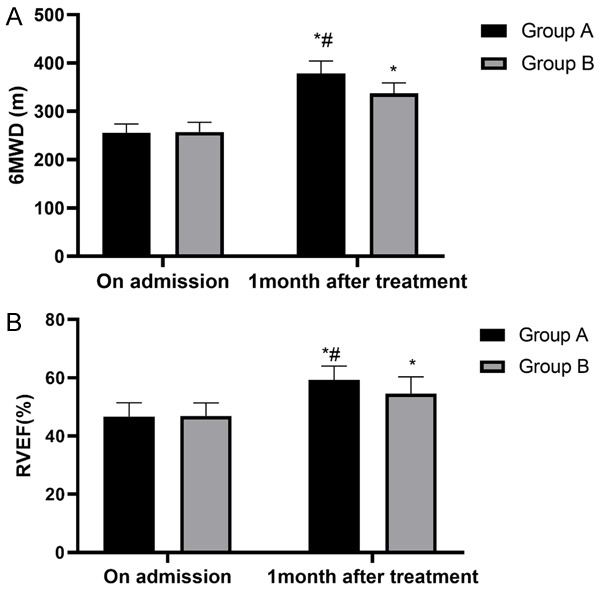
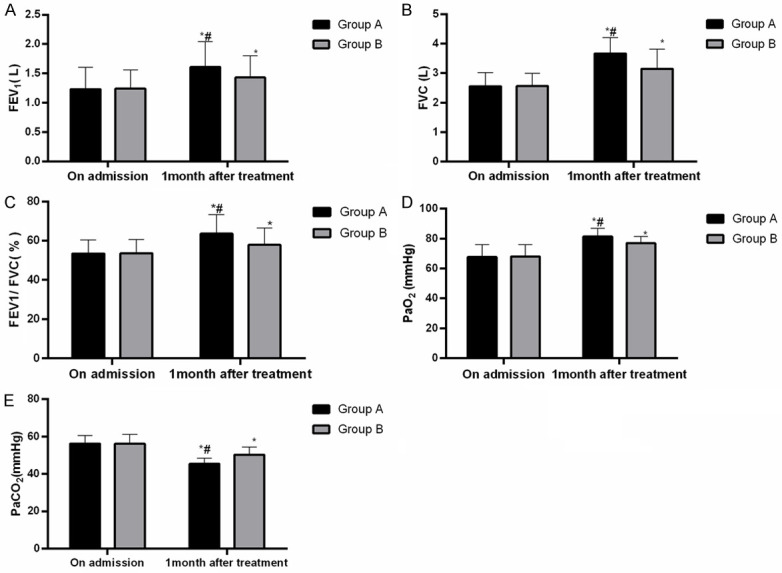
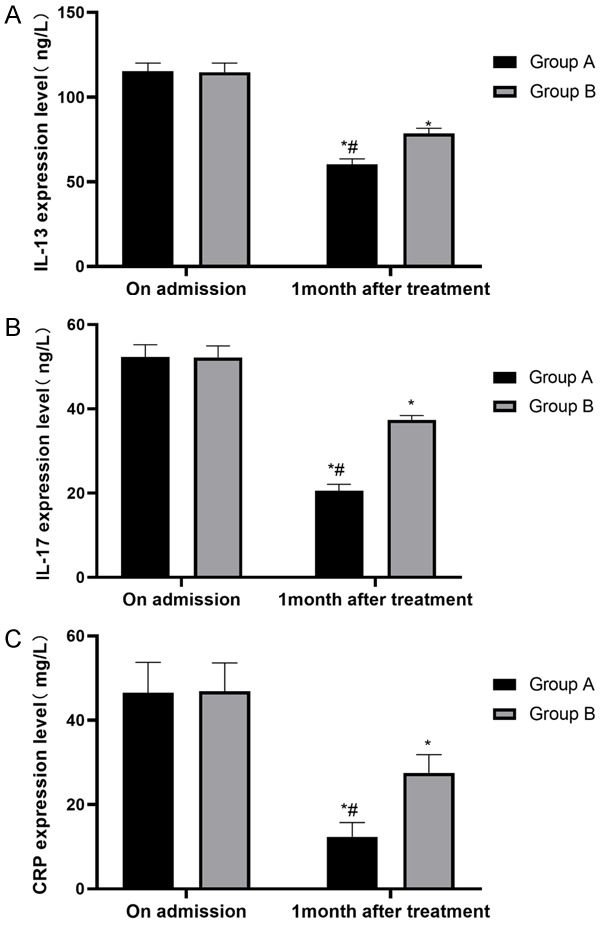
Methods: From April 2019 to October 2020, 90 COPD patients with PAH diagnosed in our hospital were recruited and divided into groups A and B. The patients in group A (50 cases) were treated with bosentan combined with sildenafil, and the patients in group B (40 cases) were administered bosentan combined with iloprost solution for inhalation. The PAH conditions, the heart rates (HR), the cardiac function, the pulmonary function, the blood gas indexes, the inflammatory factor expressions, the incidences of adverse reactions, the overall response rates (ORR), and the patient satisfaction levels were determined or evaluated.
Results: Compared with group B, the patients in group A had better recovered PAH, HR, cardiac function, pulmonary function, and blood gas indexes, lower inflammatory factor expression levels and a lower incidence of adverse reactions, as well as higher ORR and higher satisfaction levels.
Conclusion: Bosentan combined with sildenafil can reduce pulmonary artery pressure and promote the recovery of cardiopulmonary function in COPD patients with PAH.
Keywords: Chronic obstructive pulmonary disease; bosentan; pulmonary arterial hypertension; sildenafil.
AJTR Copyright © 2021.
Conflict of interest statement
None.
Figures
Similar articles
-
Acute effect of sildenafil is maintained in pulmonary arterial hypertension patients chronically treated with bosentan.Int Heart J. 2011;52(4):233-9. doi: 10.1536/ihj.52.233. Int Heart J. 2011. PMID: 21828950 Clinical Trial.
-
Fasudil reduces monocrotaline-induced pulmonary arterial hypertension: comparison with bosentan and sildenafil.Eur Respir J. 2010 Oct;36(4):800-7. doi: 10.1183/09031936.00130209. Epub 2010 Mar 29. Eur Respir J. 2010. PMID: 20351034
-
Meta-analysis of randomized controlled trials on treatment of pulmonary arterial hypertension.Circ J. 2010 Jul;74(7):1458-64. doi: 10.1253/circj.cj-09-0971. Epub 2010 Jun 1. Circ J. 2010. PMID: 20519876
-
Systematic review and cost-effectiveness of bosentan and sildenafil as therapeutic drugs for pediatric pulmonary arterial hypertension.Pediatr Pulmonol. 2021 Jul;56(7):2250-2258. doi: 10.1002/ppul.25427. Epub 2021 May 3. Pediatr Pulmonol. 2021. PMID: 33856119
-
Combined Methods (Formal Adjusted Indirect Comparison, Meta-Analysis and Principal Component Analysis) Comparisons of the Safety and Efficacy of Ambrisentan, Bosentan, and Sildenafil in the Patients With Pulmonary Arterial Hypertension.Front Pharmacol. 2020 Apr 3;11:400. doi: 10.3389/fphar.2020.00400. eCollection 2020. Front Pharmacol. 2020. PMID: 32308623 Free PMC article.
Cited by
-
Long-Term Outcome of Chronic Obstructive Pulmonary Disease: A Review.Tuberc Respir Dis (Seoul). 2022 Oct;85(4):289-301. doi: 10.4046/trd.2022.0074. Epub 2022 Jul 13. Tuberc Respir Dis (Seoul). 2022. PMID: 35822318 Free PMC article. Review.
References
-
- GBD 2015 Chronic Respiratory Disease Collaborators. Global, regional, and national deaths, prevalence, disability-adjusted life years, and years lived with disability for chronic obstructive pulmonary disease and asthma, 1990-2015: a systematic analysis for the global burden of disease study 2015. Lancet Respir Med. 2017;5:691–706. - PMC - PubMed
-
- Sood A, Assad NA, Barnes PJ, Churg A, Gordon SB, Harrod KS, Irshad H, Kurmi OP, Martin WJ 2nd, Meek P, Mortimer K, Noonan CW, Perez-Padilla R, Smith KR, Tesfaigzi Y, Ward T, Balmes J. ERS/ATS workshop report on respiratory health effects of household air pollution. Eur Respir J. 2018;51:1700698. - PMC - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous