

Cardiac Multimodality Imaging Assessment of Dystrophic Myocardial Calcification in a Human Immunodeficiency Virus-Infected Patient With Dilated Cardiomyopathy
- PMID: 34786270
- PMCID: PMC8582284
- DOI: 10.7759/cureus.18707
Cardiac Multimodality Imaging Assessment of Dystrophic Myocardial Calcification in a Human Immunodeficiency Virus-Infected Patient With Dilated Cardiomyopathy
Abstract
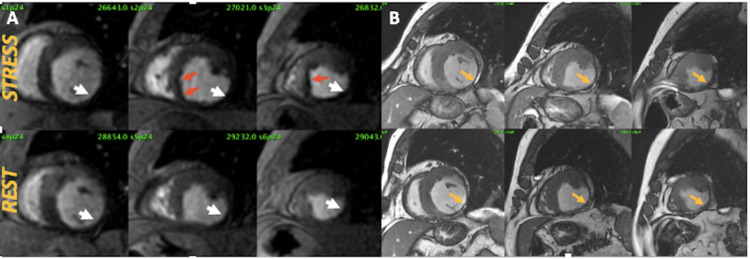
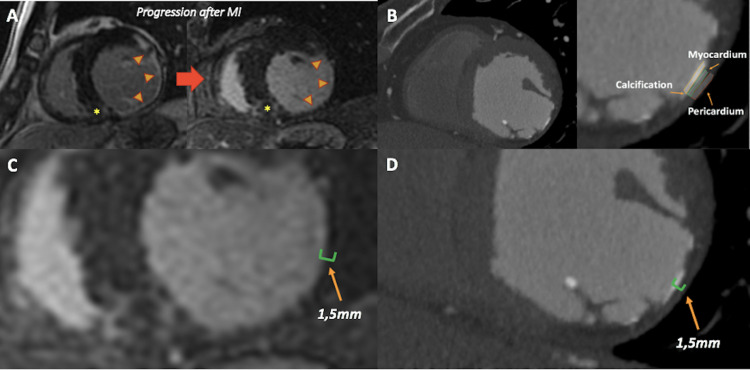
Dystrophic myocardial calcification represents the sequelae of local tissue damage and cellular necrosis. We present the case of a 72-year-old man who presented with exertional chest pain. He had a medical history of human immunodeficiency virus (HIV) infection and chronic dilated cardiomyopathy with severe left ventricular (LV) systolic dysfunction and wall motion abnormalities at the inferior and lateral LV walls. A cardiac magnetic resonance (CMR) examination from 16 years ago showed a subendocardial late gadolinium enhancement (LGE) distribution consistent with prior myocardial infarction (MI). Recently, a pharmacological stress myocardial perfusion imaging by CMR had been positive for myocardial ischemia in the left descending coronary artery (LAD) territory. A cardiac CT angiography (CCTA) showed non-significant LAD obstruction <50% consistent with microvascular ischemia and the presence of dystrophic myocardial calcification as an unusual progression of a prior MI. Conservative approach and optimal medical therapy were employed in our patient, and there was no symptom progression during the two-month follow-up period.
Keywords: cardiac multimodality imaging; dystrophic myocardial calcification; hiv-infection.
Copyright © 2021, Chango Azanza et al.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures



Similar articles
-
Multimodality imaging evaluation of Chagas disease: an expert consensus of Brazilian Cardiovascular Imaging Department (DIC) and the European Association of Cardiovascular Imaging (EACVI).Eur Heart J Cardiovasc Imaging. 2018 Apr 1;19(4):459-460n. doi: 10.1093/ehjci/jex154. Eur Heart J Cardiovasc Imaging. 2018. PMID: 29029074
-
Redefinition of uremic cardiomyopathy by contrast-enhanced cardiac magnetic resonance imaging.Kidney Int. 2006 May;69(10):1839-45. doi: 10.1038/sj.ki.5000249. Kidney Int. 2006. PMID: 16508657
-
[Late gadolinium enhancement distribution pattern of left ventricular wall in patients with dilated cardiomyopathy: a preliminary study].Zhonghua Xin Xue Guan Bing Za Zhi. 2020 Nov 24;48(11):922-929. doi: 10.3760/cma.j.cn112148-20200813-00638. Zhonghua Xin Xue Guan Bing Za Zhi. 2020. PMID: 33210863 Chinese.
-
Clinical aspects of left ventricular diastolic function assessed by Doppler echocardiography following acute myocardial infarction.Dan Med Bull. 2001 Nov;48(4):199-210. Dan Med Bull. 2001. PMID: 11767125 Review.
-
Distribution of late gadolinium enhancement in various types of cardiomyopathies: Significance in differential diagnosis, clinical features and prognosis.World J Cardiol. 2014 Jul 26;6(7):585-601. doi: 10.4330/wjc.v6.i7.585. World J Cardiol. 2014. PMID: 25068019 Free PMC article. Review.
Cited by
-
An Autopsy Case of Fulminant Myocarditis with Massive Left Ventricular Calcification.Intern Med. 2024;63(6):821-827. doi: 10.2169/internalmedicine.2200-23. Epub 2024 Mar 15. Intern Med. 2024. PMID: 38494729 Free PMC article.
-
Myocardial calcification: case reports and a systematic review.Eur Heart J Imaging Methods Pract. 2024 Jul 30;2(3):qyae079. doi: 10.1093/ehjimp/qyae079. eCollection 2024 Jul. Eur Heart J Imaging Methods Pract. 2024. PMID: 39224618 Free PMC article.
References
-
- HIV and nonischemic heart disease. Manga P, McCutcheon K, Tsabedze N, Vachiat A, Zachariah D. J Am Coll Cardiol. 2017;69:83–91. - PubMed
-
- Cardiovascular disease in HIV infection. Sudano I, Spieker LE, Noll G, Corti R, Weber R, Lüscher TF. Am Heart J. 2006;151:1147–1155. - PubMed
-
- Cardiomyopathy in AIDS: a pathophysiological perspective. Lewis W. Prog Cardiovasc Dis. 2000;43:151–170. - PubMed
-
- Myocardial calcifications: pathophysiology, etiologies, differential diagnoses, and imaging findings. Nance JW Jr, Crane GM, Halushka MK, Fishman EK, Zimmerman SL. J Cardiovasc Comput Tomogr. 2015;9:58–67. - PubMed
-
- Calcifications of the heart. Gowda RM, Boxt LM. Radiol Clin North Am. 2004;42:603–617. - PubMed
Publication types
LinkOut - more resources
Full Text Sources