

Does variability in automated perfusion software outputs for acute ischemic stroke matter? Reanalysis of EXTEND perfusion imaging
- PMID: 34786868
- PMCID: PMC8673699
- DOI: 10.1111/cns.13756
Does variability in automated perfusion software outputs for acute ischemic stroke matter? Reanalysis of EXTEND perfusion imaging
Abstract
Aims: We reprocessed the Extending the time for Thrombolysis in Emergency Neurological Deficits (EXTEND) perfusion imaging with a different automated software with the aim of comparing mismatch eligibility and outcomes.
Methods: EXTEND baseline perfusion imaging data were reprocessed using autoMIStar software to identify patients who were eligible based on the same target mismatch criteria as per the original trial.
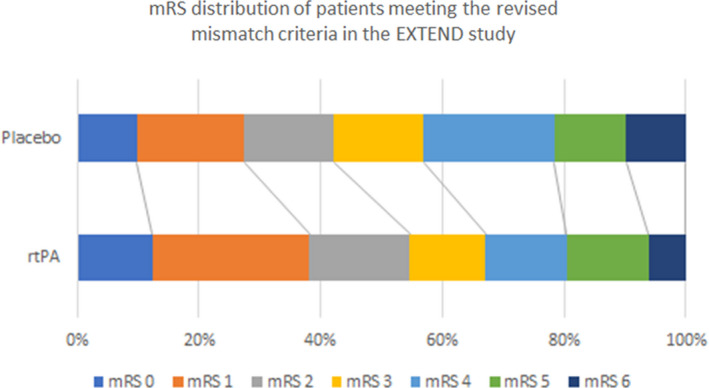
Results: From the 225 patients fulfilling RAPID-based mismatch criteria randomized in the EXTEND study, 196 (87%) patients met the revised mismatch criteria. Most common reasons for not meeting revised criteria were core >70 ml (n = 9), and no perfusion lesion/lack of penumbral tissue (n = 20). The revised perfusion lesion volumes were significantly smaller compared to the original RAPID volumes (median 68 ml IQR 34-102 ml vs. 42 ml 16-92 ml, p = 0.036). Of the patients who met the revised mismatch criteria, 40% receiving alteplase had modified Rankin Scale (mRS) 0-1 at 3-month compared to 28% with placebo (Adjusted Odds Ratio (OR) = 2.23, CI 1.08-4.58, p = 0.028). In contrast, in the original mismatch cohort, 35% receiving alteplase had mRS 0-1 at 3-month compared to 30% with placebo (adjusted OR = 1.88, p = 0.056).
Conclusions: These data reinforce the benefit of alteplase in the later time window, and suggest that differences in automated perfusion imaging software outputs may be clinically relevant.
Trial registration: ClinicalTrials.gov NCT00887328 NCT01580839.
Keywords: CT perfusion; ischemic stroke; target mismatch; thrombolysis.
© 2021 The Authors. CNS Neuroscience & Therapeutics Published by John Wiley & Sons Ltd.
Conflict of interest statement
Dr. Davis, receiving advisory board fees from AstraZeneca and Boehringer Ingelheim; and Dr. Donnan, receiving advisory board fees from AstraZeneca Australia, Bayer, Boehringer Ingelheim, Merck, Pfizer, and Servier; Dr. Parsons reports receiving advisory board fees from Boehringer Ingelheim, and research partnerships with Canon Medical Systems, Apollo Medical Imaging, and Siemens. No other potential conflict of interest relevant to this article were reported.
Figures
References
-
- Nogueira RG, Jadhav AP, Haussen DC, et al. Thrombectomy 6 to 24 Hours after Stroke with a Mismatch between Deficit and Infarct. N Engl J Med. 2018;378:11‐21. - PubMed
-
- Ma H, Campbell BCV, Parsons MW, et al. Thrombolysis guided by perfusion imaging up to 9 hours after onset of stroke. N Engl J Med. 2019;380:1795‐1803. - PubMed
-
- Campbell BC, Christensen S, Levi CR, et al. Cerebral blood flow is the optimal CT perfusion parameter for assessing infarct core. Stroke; J Cereb Circ. 2011;42:3435‐3440. - PubMed
-
- Bivard A, Spratt N, Levi C, Parsons M. Perfusion computer tomography: imaging and clinical validation in acute ischaemic stroke. Brain: J Neurol. 2011;134:3408‐3416. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
