

Pathogenesis of Respiratory Viral and Fungal Coinfections
- PMID: 34788127
- PMCID: PMC8597983
- DOI: 10.1128/CMR.00094-21
Pathogenesis of Respiratory Viral and Fungal Coinfections
Abstract
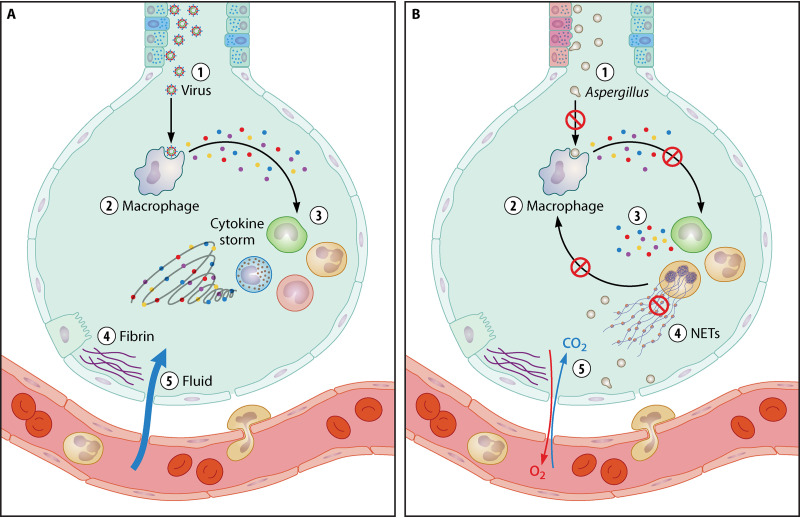
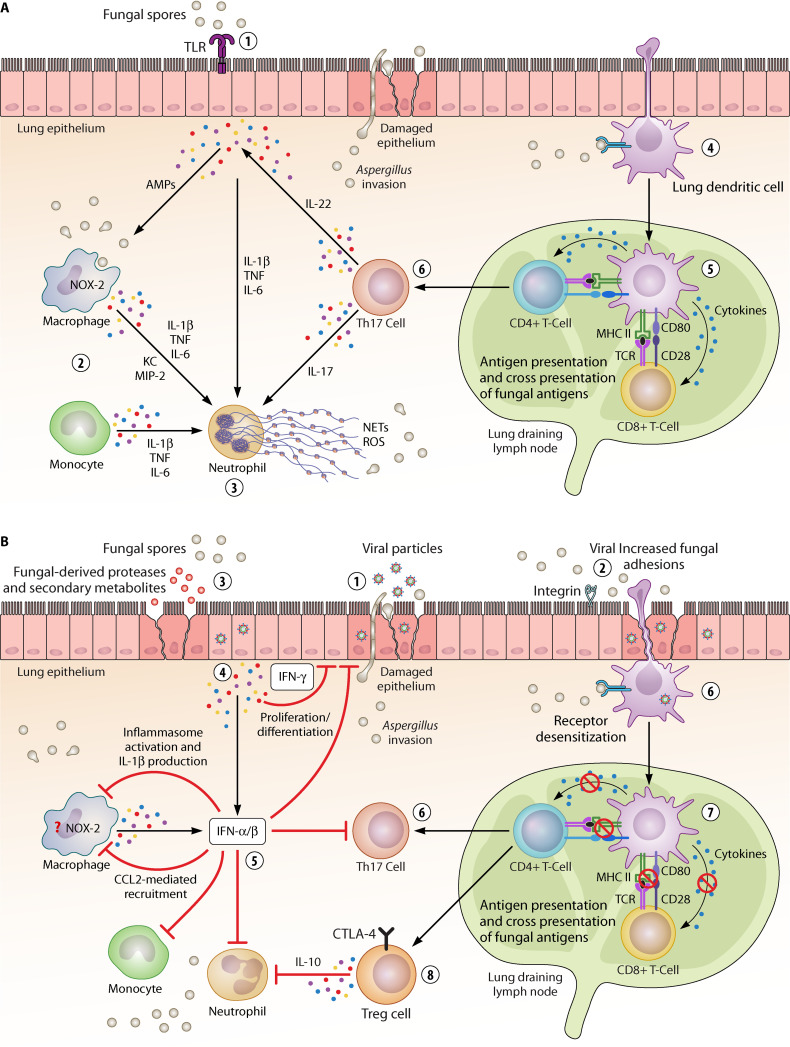
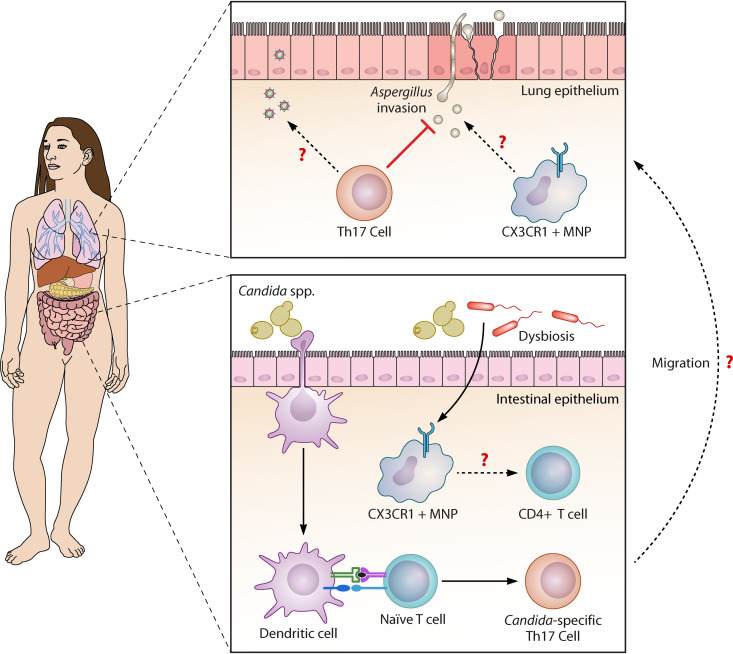
Individuals suffering from severe viral respiratory tract infections have recently emerged as "at risk" groups for developing invasive fungal infections. Influenza virus is one of the most common causes of acute lower respiratory tract infections worldwide. Fungal infections complicating influenza pneumonia are associated with increased disease severity and mortality, with invasive pulmonary aspergillosis being the most common manifestation. Strikingly, similar observations have been made during the current coronavirus disease 2019 (COVID-19) pandemic. The copathogenesis of respiratory viral and fungal coinfections is complex and involves a dynamic interplay between the host immune defenses and the virulence of the microbes involved that often results in failure to return to homeostasis. In this review, we discuss the main mechanisms underlying susceptibility to invasive fungal disease following respiratory viral infections. A comprehensive understanding of these interactions will aid the development of therapeutic modalities against newly identified targets to prevent and treat these emerging coinfections.
Keywords: SARS-CoV; antifungal immunity; aspergillosis; coinfection; copathogenesis; fungal pathogens; influenza; respiratory viruses.
Figures
References
-
- White PL, Dhillon R, Cordey A, Hughes H, Faggian F, Soni S, Pandey M, Whitaker H, May A, Morgan M, Wise MP, Healy B, Blyth I, Price JS, Vale L, Posso R, Kronda J, Blackwood A, Rafferty H, Moffitt A, Tsitsopoulou A, Gaur S, Holmes T, Backx M. 2020. A national strategy to diagnose COVID-19 associated invasive fungal disease in the ICU. Clin Infect Dis 73:e1634–e1644. 10.1093/cid/ciaa1298. - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
