

A randomized controlled study of convalescent plasma for individuals hospitalized with COVID-19 pneumonia
- PMID: 34788233
- PMCID: PMC8670841
- DOI: 10.1172/JCI155114
A randomized controlled study of convalescent plasma for individuals hospitalized with COVID-19 pneumonia
Abstract
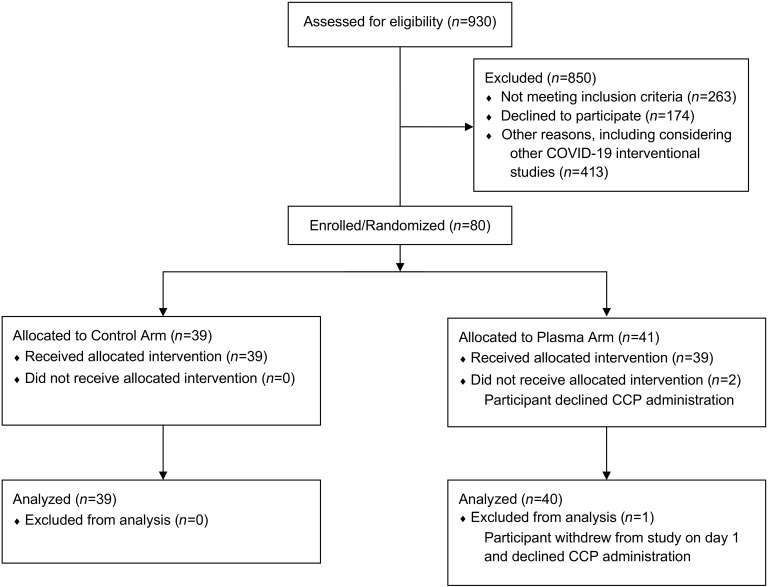
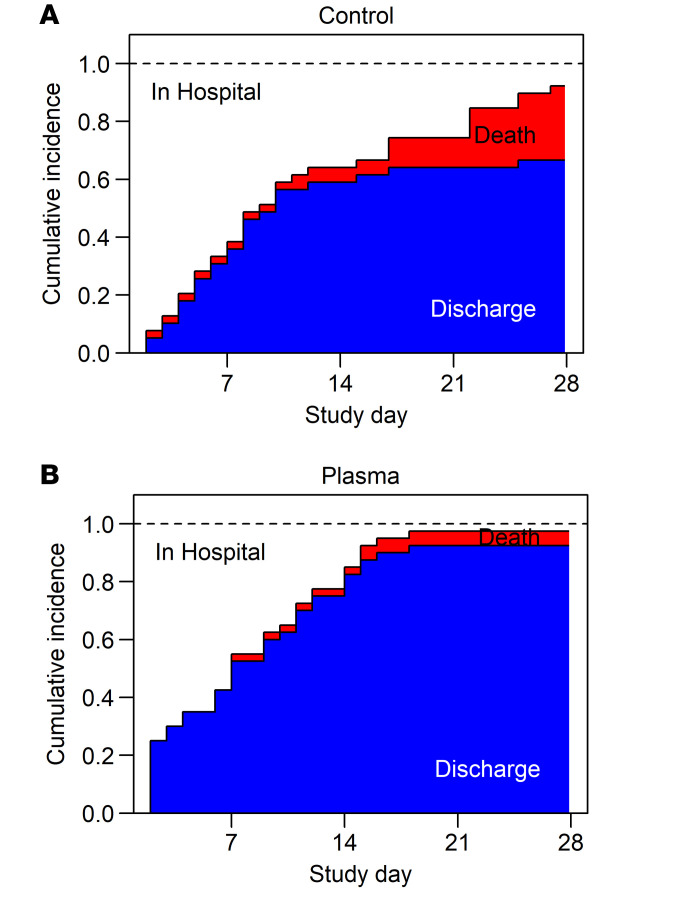
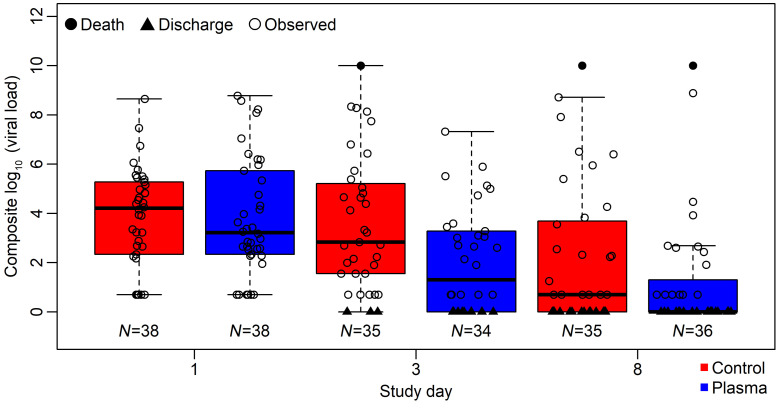
BackgroundAntibody-based strategies for COVID-19 have shown promise in prevention and treatment of early disease. COVID-19 convalescent plasma (CCP) has been widely used but results from randomized trials supporting its benefit in hospitalized patients with pneumonia are limited. Here, we assess the efficacy of CCP in severely ill, hospitalized adults with COVID-19 pneumonia.MethodsWe performed a randomized control trial (PennCCP2), with 80 adults hospitalized with COVID-19 pneumonia, comparing up to 2 units of locally sourced CCP plus standard care versus standard care alone. The primary efficacy endpoint was comparison of a clinical severity score. Key secondary outcomes include 14- and 28-day mortality, 14- and 28-day maximum 8-point WHO ordinal score (WHO8) score, duration of supplemental oxygenation or mechanical ventilation, respiratory SARS-CoV-2 RNA, and anti-SARS-CoV-2 antibodies.ResultsEighty hospitalized adults with confirmed COVID-19 pneumonia were enrolled at median day 6 of symptoms and day 1 of hospitalization; 60% were anti-SARS-CoV-2 antibody seronegative. Participants had a median of 3 comorbidities, including risk factors for severe COVID-19 and immunosuppression. CCP treatment was safe and conferred significant benefit by clinical severity score (median [MED] and interquartile range [IQR] 10 [5.5-30] vs. 7 [2.75-12.25], P = 0.037) and 28-day mortality (n = 10, 26% vs. n = 2, 5%; P = 0.013). All other prespecified outcome measures showed weak evidence toward benefit of CCP.ConclusionTwo units of locally sourced CCP administered early in hospitalization to majority seronegative participants conferred a significant benefit in clinical severity score and 28-day mortality. Results suggest CCP may benefit select populations, especially those with comorbidities who are treated early.Trial RegistrationClinicalTrials.gov NCT04397757.FundingUniversity of Pennsylvania.
Keywords: Adaptive immunity; COVID-19; Clinical Trials.
Conflict of interest statement
Figures
References
-
- Worldometers.info. https://www.worldometers.info/coronavirus/ Updated November 1, 2021. Accessed November 1, 2021.
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
