

Randomized Controlled Trial
doi: 10.1164/rccm.202105-1212LE.
Phenotypes of Patients with COVID-19 Who Have a Positive Clinical Response to Helmet Noninvasive Ventilation
Collaborators,
Affiliations
- PMID: 34788583
- PMCID: PMC8887003
- DOI: 10.1164/rccm.202105-1212LE
Item in Clipboard
Randomized Controlled Trial
Phenotypes of Patients with COVID-19 Who Have a Positive Clinical Response to Helmet Noninvasive Ventilation
Am J Respir Crit Care Med.
.
No abstract available
Figures
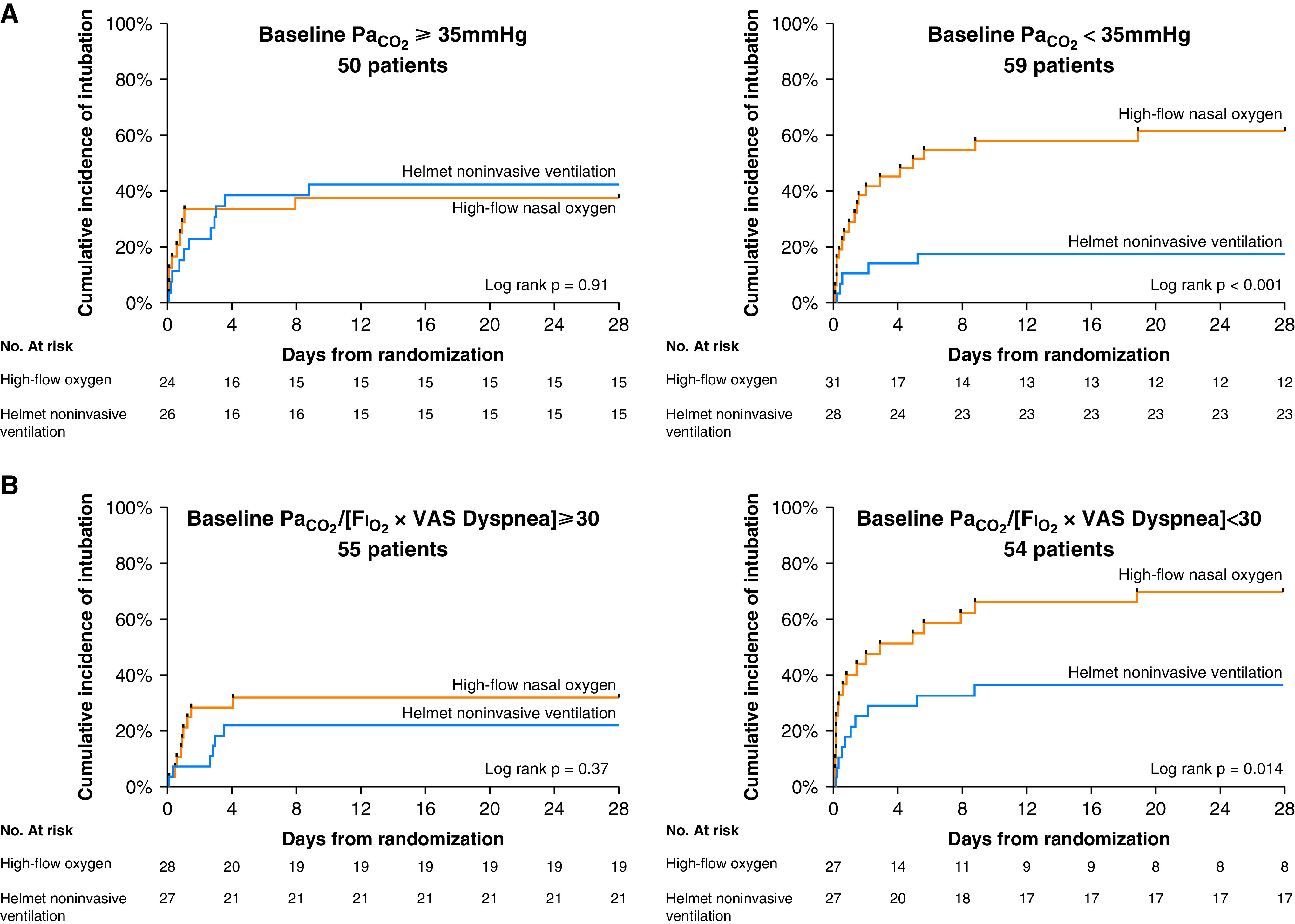
(A) Kaplan-Meier plots of the cumulative incidence of intubation from randomization to Day 28 in the subgroup of patients with PaCO2 of less than 35 mm Hg (n = 59 patients) and 35 mm Hg or more (n = 50 patients) at study enrollment. The hazard ratio for endotracheal intubation in the helmet noninvasive ventilation group in patients with PaCO2 of less than 35 mm Hg was 0.25 (95% CI, 0.11–0.57). The hazard ratio for endotracheal intubation in the helmet noninvasive ventilation group in patients with PaCO2 of at least 35 mm Hg was 1.05 (95% CI, 0.44–2.53). (B) Kaplan-Meier plots of the cumulative incidence of intubation from randomization to Day 28 in the subgroup of patients with PaO2/(Fi O2 × dyspnea) lower (n = 54 patients) and equal to or higher than (n = 55 patients) 30 at study enrollment. The hazard ratio for endotracheal intubation in the helmet noninvasive ventilation group in patients with PaO2/(Fi O2 × VAS dyspnea) < 30 was 0.39 (95% CI, 0.19–0.82). The hazard ratio for endotracheal intubation in the helmet noninvasive ventilation group in patients with PaO2/(Fi O2 × VAS dyspnea) ⩾ 30 was 0.63 (95% CI, 0.23–1.73). CI = confidence interval; VAS = visual analog scale.
References
-
- Grieco DL, Menga LS, Cesarano M, Rosà T, Spadaro S, Bitondo MM, et al. COVID-ICU Gemelli Study Group Effect of helmet noninvasive ventilation vs high-flow nasal oxygen on days free of respiratory support in patients with COVID-19 and moderate to severe hypoxemic respiratory failure: the HENIVOT randomized clinical trial. JAMA . 2021;325:1731–1743. - PMC - PubMed
-
- Munshi L, Hall JB. Respiratory support during the COVID-19 pandemic: is it time to consider using a helmet? JAMA . 2021;325:1723–1725. - PubMed
-
- Roca O, Caralt B, Messika J, Samper M, Sztrymf B, Hernández G, et al. An index combining respiratory rate and oxygenation to predict outcome of nasal high-flow therapy. Am J Respir Crit Care Med . 2019;199:1368–1376. - PubMed
-
- Dres M, Similowski T, Goligher EC, Pham T, Sergenyuk L, Telias I, et al. Dyspnoea and respiratory muscle ultrasound to predict extubation failure. Eur Respir J . 2021;58:2100002. - PubMed
-
- Dangers L, Montlahuc C, Kouatchet A, Jaber S, Meziani F, Perbet S, et al. REVA Network (Research Network in Mechanical Ventilation) and the Groupe de Recherche en Réanimation Respiratoire en Onco-Hématologie (GrrrOH) List of contributors who included study patients: Angers University Hospital, Angers, France. Dyspnoea in patients receiving noninvasive ventilation for acute respiratory failure: prevalence, risk factors and prognostic impact: a prospective observational study. Eur Respir J . 2018;52:1702637. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
