

Aspergillus-related lung disease in people with cystic fibrosis: can imaging help us to diagnose disease?
- PMID: 34789463
- PMCID: PMC9488454
- DOI: 10.1183/16000617.0103-2021
Aspergillus-related lung disease in people with cystic fibrosis: can imaging help us to diagnose disease?
Abstract
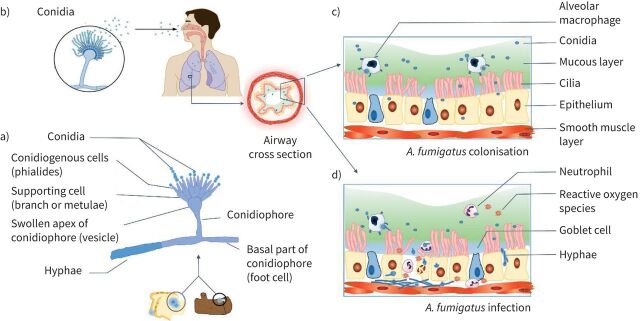
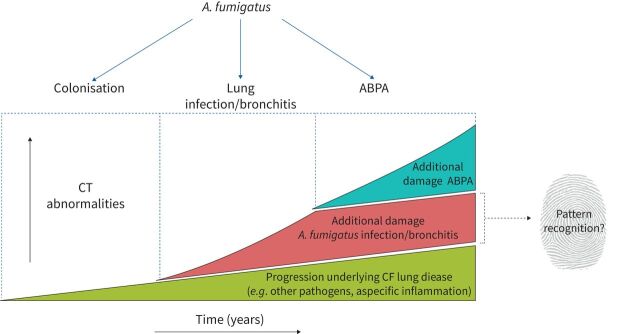
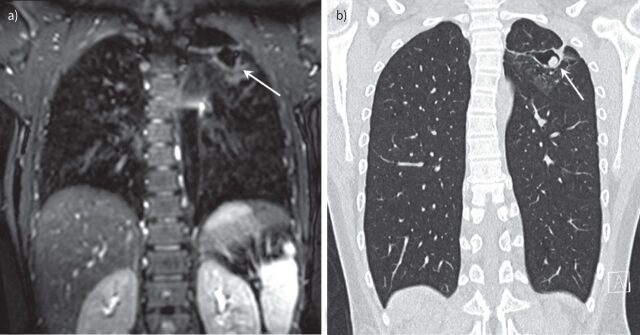
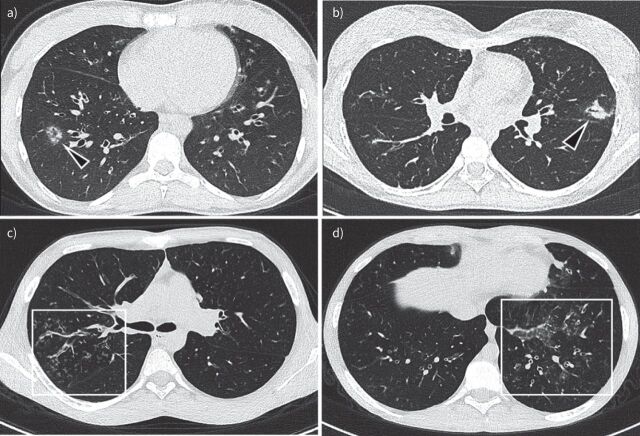
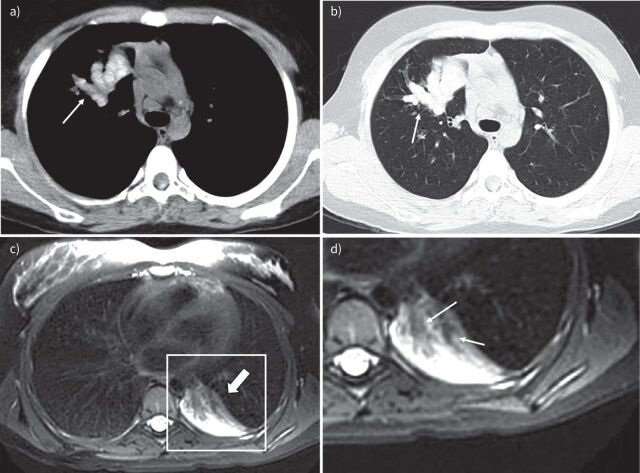
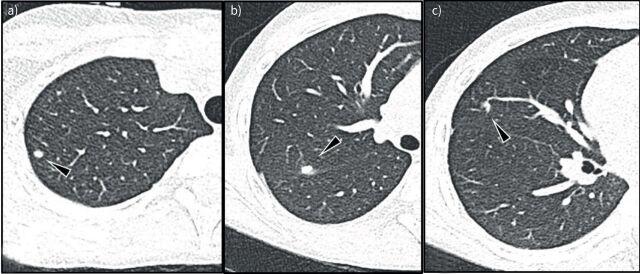
In people with cystic fibrosis (PwCF), viscous sputum and dysfunction of the mucociliary escalator leads to early and chronic infections. The prevalence of Aspergillus fumigatus in sputum is high in PwCF and the contribution of A. fumigatus to the progression of structural lung disease has been reported. However, overall, relatively little is known about the contribution of A. fumigatus to CF lung disease. More knowledge is needed to aid clinical decisions on whether to start antifungal treatment. In this review, we give an overview of A. fumigatus colonisation and infection in PwCF and the different types of pulmonary disease caused by it. Furthermore, we discuss the current evidence for structural lung damage associated with A. fumigatus in PwCF on chest computed tomography and magnetic resonance imaging. We conclude that radiological outcomes to identify disease caused by A. fumigatus can be important for clinical studies and management.
Copyright ©The authors 2021.
Conflict of interest statement
Conflict of interest: Q. Lv has nothing to disclose. Conflict of interest: B.B.L.J. Elders has nothing to disclose. Conflict of interest: A. Warris has nothing to disclose. Conflict of interest: D. Caudri has nothing to disclose. Conflict of interest: P. Ciet reports personal fees from Vertex Pharmaceutical, outside the submitted work. Conflict of interest: H. Tiddens reports grants and other funding from Novartis, grants from CFF and Vectura, and personal fees from Vertex, Thirona and Insmed, outside the submitted work. In addition, Erasmus MC and Telethon Kids Institute have licensed the use of PRAGMA-CF to Thirona and Resonance Health. The Sophia research BV of the Erasmus MC-Sophia Childrens hospital has received unconditional research grants from Novartis, and Vectura.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical