

Organoid Sensitivity Correlates with Therapeutic Response in Patients with Pancreatic Cancer
- PMID: 34789479
- PMCID: PMC8866201
- DOI: 10.1158/1078-0432.CCR-20-4116
Organoid Sensitivity Correlates with Therapeutic Response in Patients with Pancreatic Cancer
Abstract
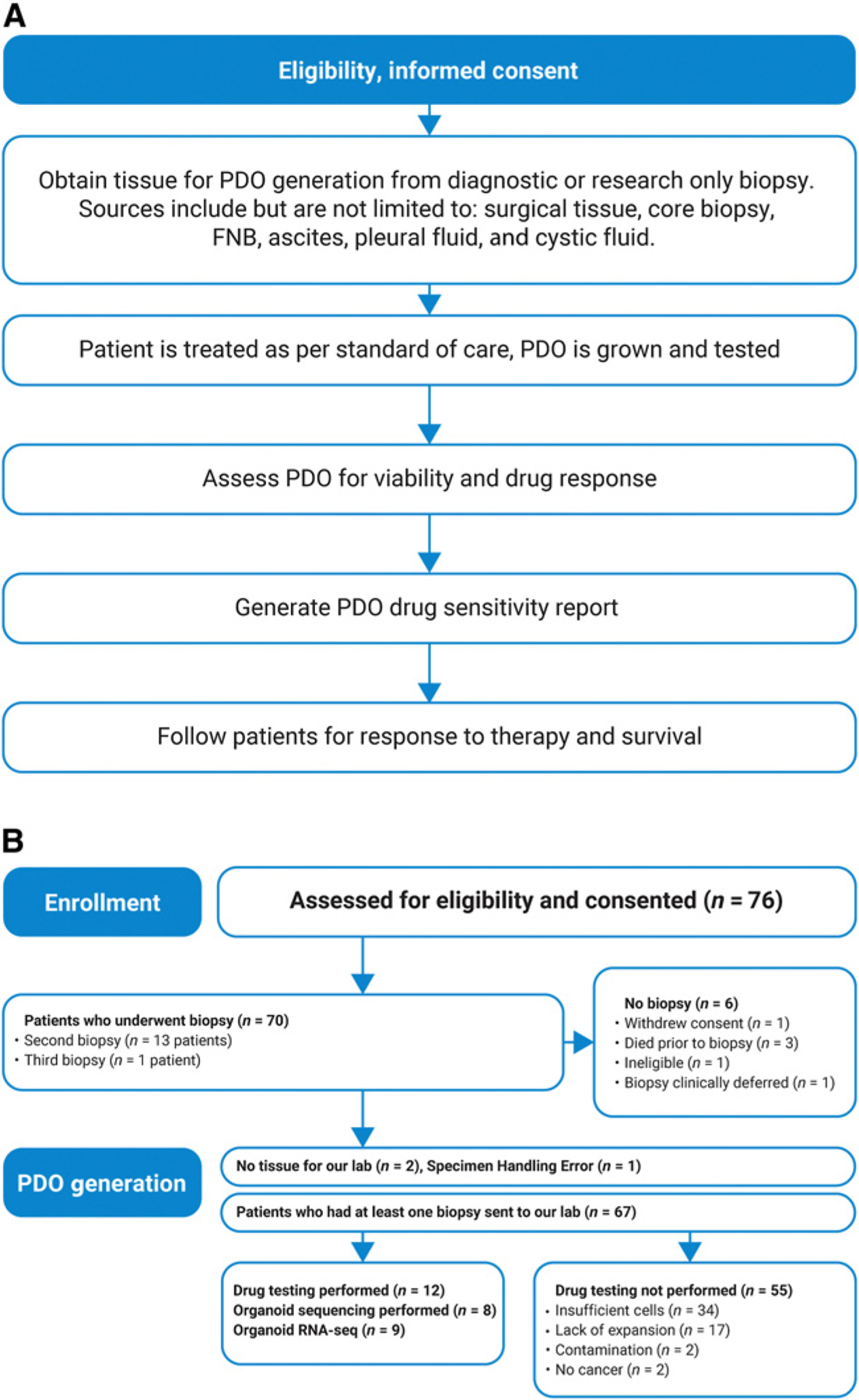
Purpose: Pancreatic ductal adenocarcinoma (PDAC) remains a significant health issue. For most patients, there are no options for targeted therapy, and existing treatments are limited by toxicity. The HOPE trial (Harnessing Organoids for PErsonalized Therapy) was a pilot feasibility trial aiming to prospectively generate patient-derived organoids (PDO) from patients with PDAC and test their drug sensitivity and correlation with clinical outcomes.
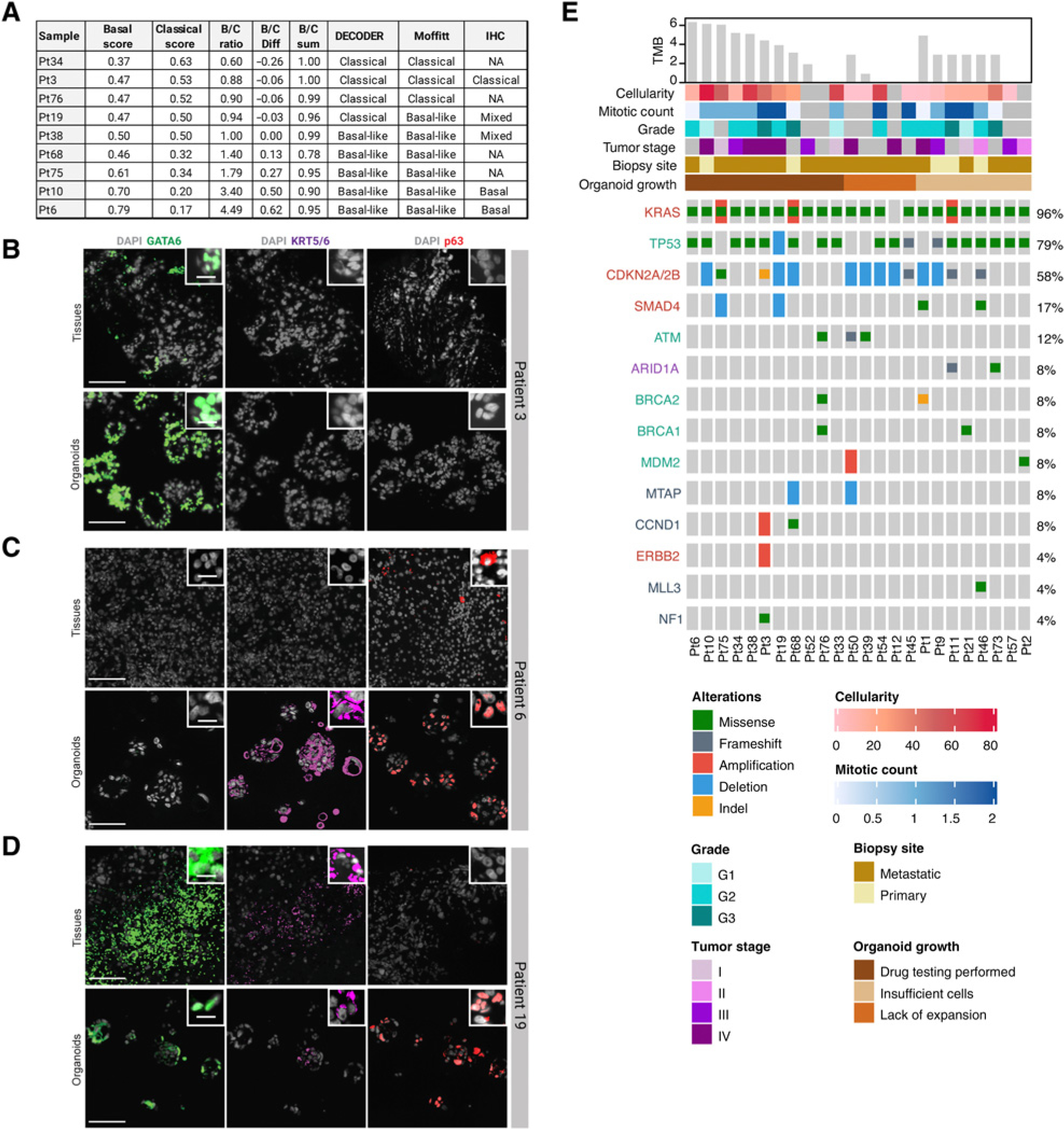
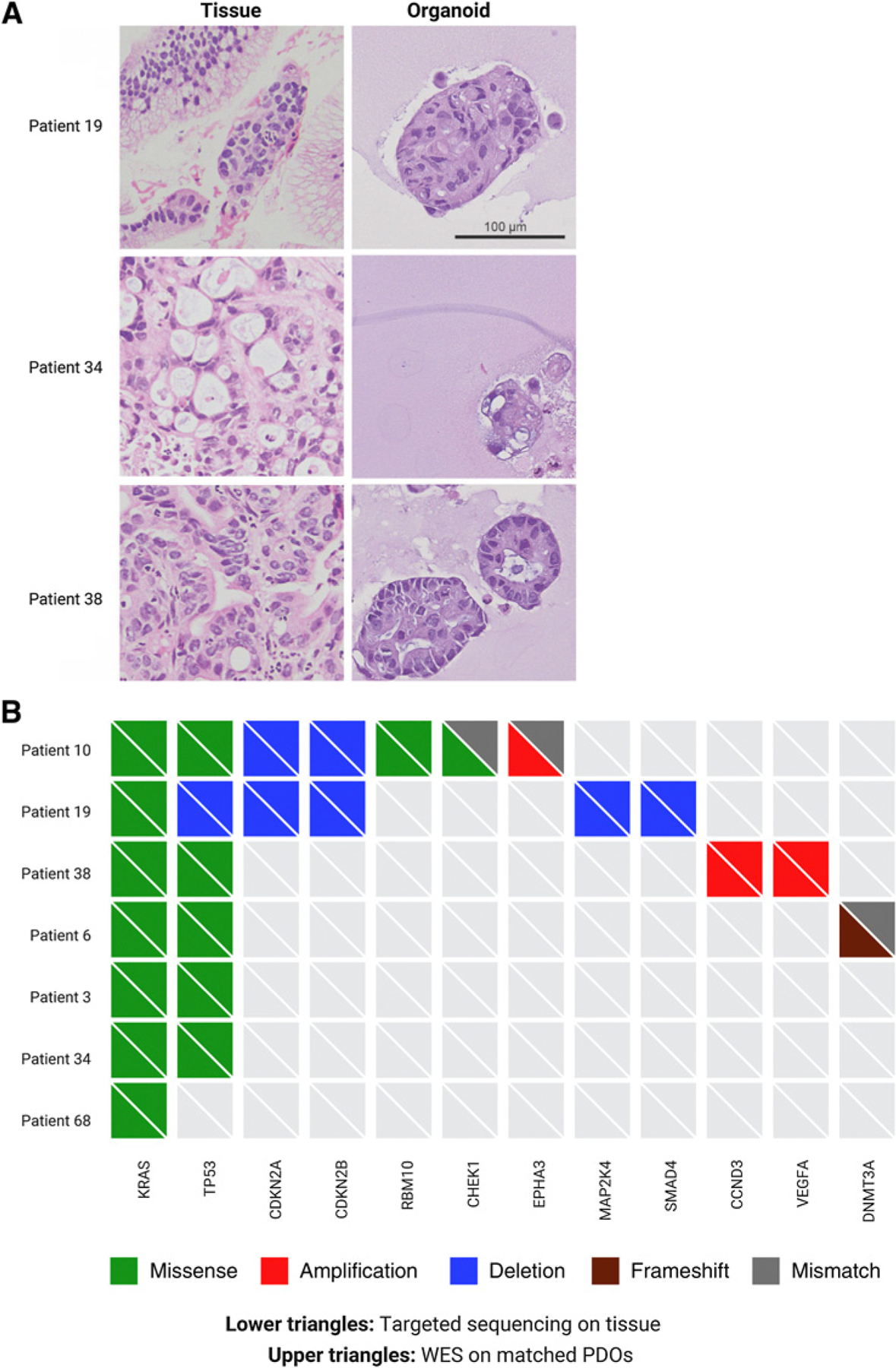
Experimental design: PDOs were established from a heterogeneous population of patients with PDAC including both basal and classical PDAC subtypes.
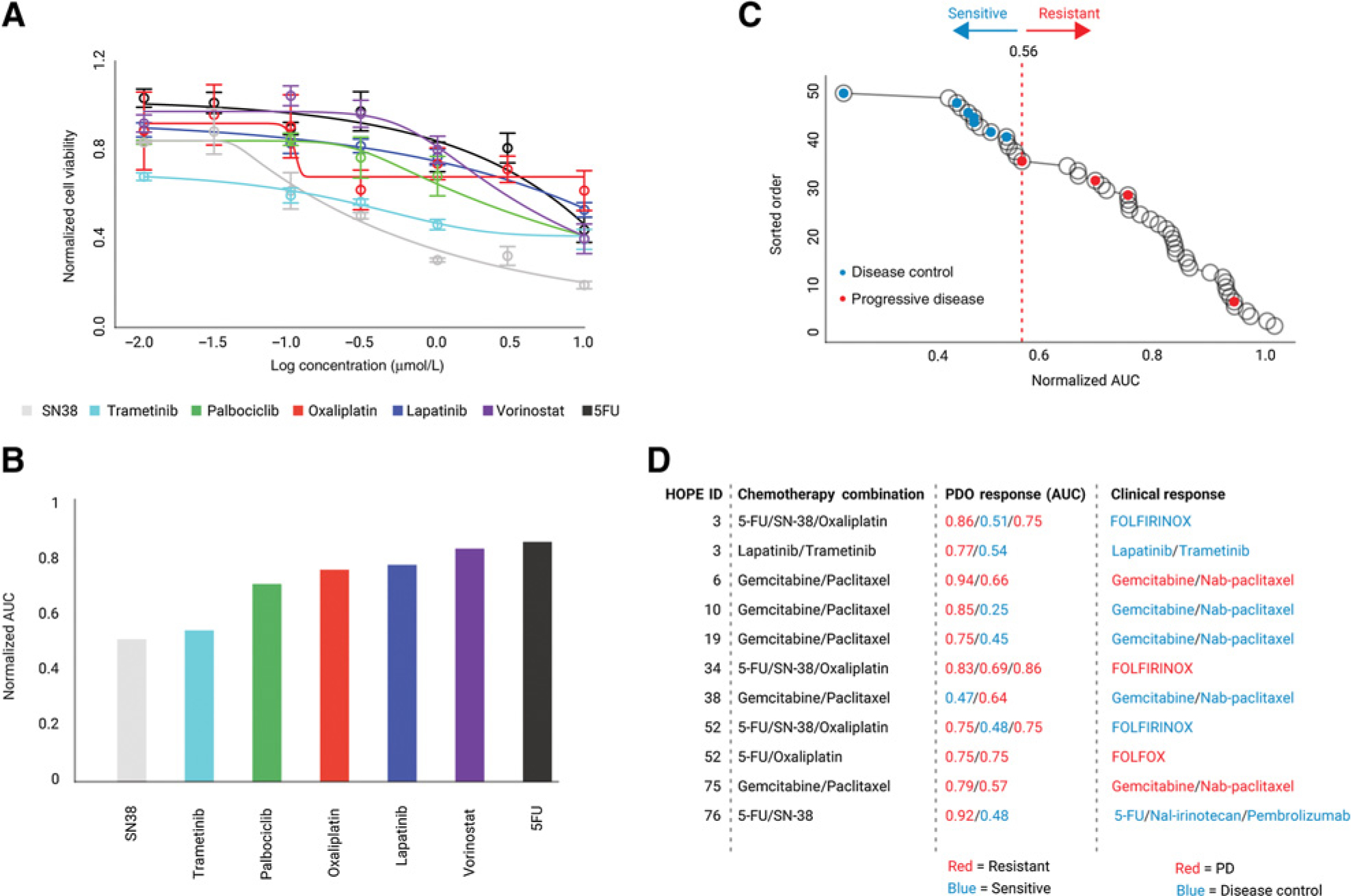
Results: A method for classifying PDOs as sensitive or resistant to chemotherapy regimens was developed to predict the clinical outcome of patients. Drug sensitivity testing on PDOs correlated with clinical responses to treatment in individual patients.
Conclusions: These data support the investigation of PDOs to guide treatment in prospective interventional trials in PDAC.
©2021 American Association for Cancer Research.
Figures
References
-
- Tempero MA. NCCN guidelines updates: pancreatic cancer. J Natl Compr Canc Netw 2019;17:603–5. - PubMed
-
- Ettinger DS, Aisner DL, Wood DE, Akerley W, Bauman J, Chang JY, et al. NCCN guidelines insights: non-small cell lung cancer, version 5.2018. J Natl Compr Canc Netw 2018;16:807–21. - PubMed
-
- Biankin AV, Maitra A. Subtyping pancreatic cancer. Cancer Cell 2015;28:411–3. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
