

Time-Based Decision Making for Reperfusion in Acute Ischemic Stroke
- PMID: 34790159
- PMCID: PMC8591257
- DOI: 10.3389/fneur.2021.728012
Time-Based Decision Making for Reperfusion in Acute Ischemic Stroke
Abstract
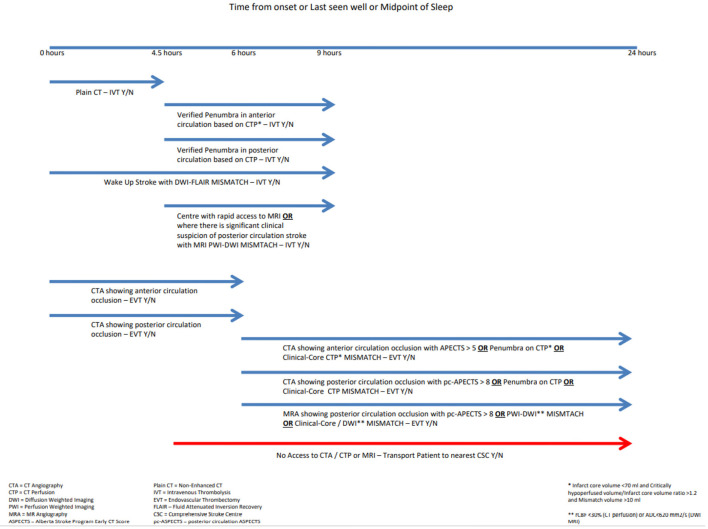
Decision making in the extended time windows for acute ischemic stroke can be a complex and time-consuming process. The process of making the clinical decision to treat has been compounded by the availability of different imaging modalities. In the setting of acute ischemic stroke, time is of the essence and chances of a good outcome diminish by each passing minute. Navigating the plethora of advanced imaging modalities means that treatment in some cases can be inefficaciously delayed. Time delays and individually based non-programmed decision making can prove challenging for clinicians. Visual aids can assist such decision making aimed at simplifying the use of advanced imaging. Flow charts are one such visual tool that can expedite treatment in this setting. A systematic review of existing literature around imaging modalities based on site of occlusion and time from onset can be used to aid decision making; a more program-based thought process. The use of an acute reperfusion flow chart helping navigate the myriad of imaging modalities can aid the effective treatment of patients.
Keywords: acute ischaemia; computer tomography (CT); magnetic resonance imaging (MRI); stroke; thrombectomy; thrombolysis.
Copyright © 2021 Grøan, Ospel, Ajmi, Sandset, Kurz, Skjelland and Advani.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures


References
-
- Powers WJ, Rabinstein AA, Ackerson T, Adeoye OM, Bambakidis NC, Becker K, et al. . 2018 Guidelines for the early management of patients with acute ischemic stroke: a guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. (2018) 49:e46–110. 10.1161/STR.0000000000000163 - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources