

Favorable tumor biology in locally advanced pancreatic cancer-beyond CA19-9
- PMID: 34790409
- PMCID: PMC8576224
- DOI: 10.21037/jgo-20-426
Favorable tumor biology in locally advanced pancreatic cancer-beyond CA19-9
Abstract
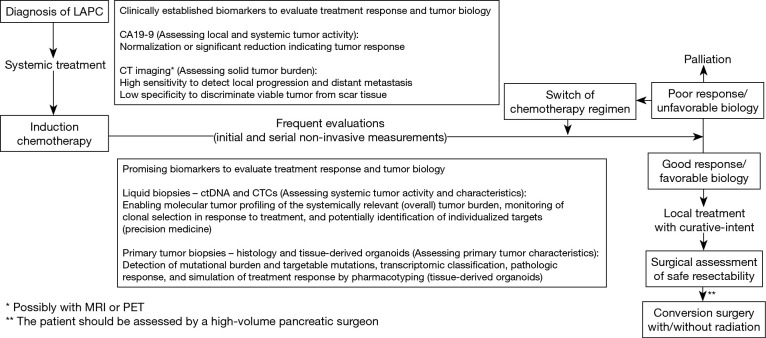
Patients with pancreatic ductal adenocarcinoma (PDAC) are frequently staged as unresectable locally advanced pancreatic cancer (LAPC) at the time of diagnosis. Recently, the administration of multi-agent induction chemotherapy has resulted in treatment response in up to 60% of these patients rendering their tumors technically resectable. Operative strategies have evolved to allow for successful oncologic resection of LAPC. These technically complex procedures involving vascular resections and reconstructions are now being performed with increasing safety at high-volume centers. However, even after induction therapy and successful resection, disease recurrence sometimes occurs early on, limiting the benefit of resecting the local tumor. Therefore, selection of surgical candidates should factor in each patient's tumor biology which could result in accurate treatment guidance to improve patient outcomes while avoiding overtreatment. Well-informed patient selection is critical to improve outcomes in LAPC. Multidisciplinary teams have to determine the appropriate care for LAPC patients at the time of reevaluation after administration of induction chemotherapy. At this point the concept of favorable vs. unfavorable tumor biology becomes highly relevant and having access to biomarkers that are predictive of tumor behavior are of paramount importance. Currently, CA19-9 remains the only clinically utilized biomarker for PDAC, however, its use is limited by factors discussed in this review. While CA19-9 holds value in patient assessment, additional biomarkers are required that could supplement and improve the current ability to classify tumor biology and predict behavior in individual patients. Recent investigations on the use of circulating tumor DNA (ctDNA) and circulating tumor cells (CTCs) using liquid biopsies, as well as patient-derived organoids to characterize tumor biology have shown promise in achieving precise tumor biology-based patient stratification. Serial assessment of these biomarkers throughout therapy could supplement or even replace the anatomic criteria for resectability in the future.
Keywords: Pancreatic surgery; circulating tumor cells (CTCs); induction chemotherapy; neoadjuvant chemotherapy; recurrence.
2021 Journal of Gastrointestinal Oncology. All rights reserved.
Conflict of interest statement
Conflicts of Interest: All authors have completed the ICMJE uniform disclosure form (available at http://dx.doi.org/10.21037/jgo-20-426). The series “Surgery for Locally Advanced Pancreatic Cancer” was commissioned by the editorial office without any funding or sponsorship. The authors have no other conflicts of interest to declare.
Figures
References
Publication types
LinkOut - more resources
Full Text Sources