

Common bile duct size in malignant distal obstruction and lumen-apposing metal stents: a multicenter prospective study
- PMID: 34790548
- PMCID: PMC8589552
- DOI: 10.1055/a-1526-1208
Common bile duct size in malignant distal obstruction and lumen-apposing metal stents: a multicenter prospective study
Abstract
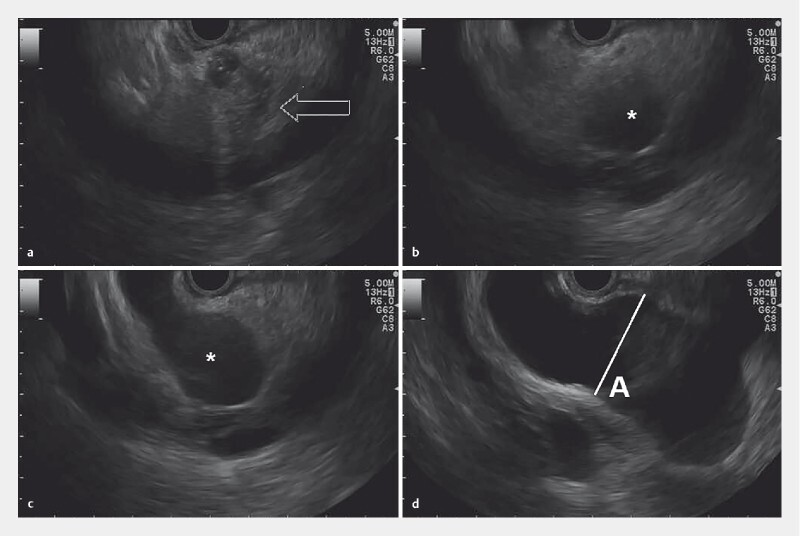
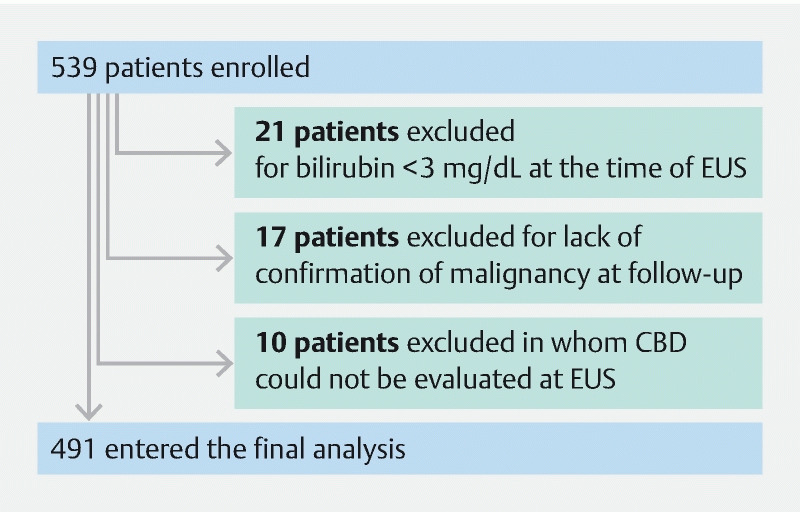
Background and study aims Feasibility of EUS-guided choledochoduodenostomy (EUS-CDS) using available lumen-apposing stents (LAMS) is limited by the size of the common bile duct (CBD) (≤ 12 mm, cut-off for experts; 15 mm, cut-off for non-experts). We aimed to assess the prevalence and predictive factors associated with CBD size ≥ 12 and 15 mm in naïve patients with malignant distal biliary obstruction (MDBO). Patients and methods This was a prospective cohort study involving 22 centers with assessment of CBD diameter and subjective feasibility of the EUS-CDS performance in naïve jaundiced patients undergoing EUS evaluation for MDBO. Results A total of 491 patients (mean age 69 ± 12 years) with mean serum bilirubin of 12.7 ± 6.6 mg/dL entered the final analysis. Dilation of the CBD ≥ 12 and 15 mm was detected in 78.8 % and 51.9 % of cases, respectively. Subjective feasibility of EUS-CDS was expressed by endosonographers in 91.2 % for a CBD ≥ 12 mm and in 96.5 % for a CBD ≥ 15 mm. On multivariate analysis, age ( P < 0.01) and bilirubin level ( P ≤ 0.001) were the only factors associated with both CBD dilation ≥ 12 and ≥ 15 mm. These variables were poorly associated with the extent of duct dilation; however, based on them a prediction model could be constructed that satisfactorily predicted CBD size ≥ 12 mm in patients at least 70 years and a bilirubin level ≥ 7 mg/dL. Conclusions Our study showed that at presentation in a large cohort of patients with MDBO, EUS-CDS can be potentially performed in three quarters to half of cases by expert and less experienced endosonographers, respectively. Dedicated stents or devices with different designs able to overcome the limitations of existing electrocautery-enhanced LAMS for EUS-CDS are needed.
The Author(s). This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/).
Conflict of interest statement
Competing interests Dr. Anderloni is a consultant for Boston Scientific, Olympus Medical and Medtronic. Dr. Fabbri is a consultant for Boston Scientific. Dr. Napoleon has held supported teaching sessions and had research collaboration with Boston Scientific. Dr. Poley served as a consultant for and received speaker and travel fees from Boston Scientific, Cook Endoscopy, and Pentax. Dr. Mutignani had a research collaboration with Boston Scientific. Dr. Palazzo is a consultant for Boston Scientific. Dr. Itoi is a speaker for Boston Scientific. Dr. Costamagna received research support from Cook Endoscopy and he currently is a member of Advisory Committees or review panels for Olympus Medical and Boston Scientific. Dr. Larghi received educational fees from Boston Scientific and Pentax.
Figures

References
-
- Boulay B R, Lo S K. Endoscopic ultrasound-guided biliary drainage. Gastrointest Endosc Clin N Am. 2018;28:171–185. - PubMed
-
- Sharaiha R Z, Khan M A, Kamal F et al. Efficacy and safety of EUS-guided biliary drainage in comparison with percutaneous biliary drainage when ERCP fails: a systematic review and meta-analysis. Gastrointest Endosc. 2017;85:904–914. - PubMed
-
- Park J K, Woo Y S, Noh D H et al. Efficacy of EUS-guided and ERCP-guided biliary drainage for malignant biliary obstruction: prospective randomized controlled study. Gastrointest Endosc. 2018;88:277–282. - PubMed
-
- Bang J Y, Navaneethan U, Hasan M et al. Stent placement by EUS or ERCP for primary biliary decompression in pancreatic cancer: a randomized trial (with videos) Gastrointest Endosc. 2018;88:9–17. - PubMed
LinkOut - more resources
Full Text Sources