

Refractory Gastroesophageal Reflux Disease: A Management Update
- PMID: 34790683
- PMCID: PMC8591082
- DOI: 10.3389/fmed.2021.765061
Refractory Gastroesophageal Reflux Disease: A Management Update
Abstract
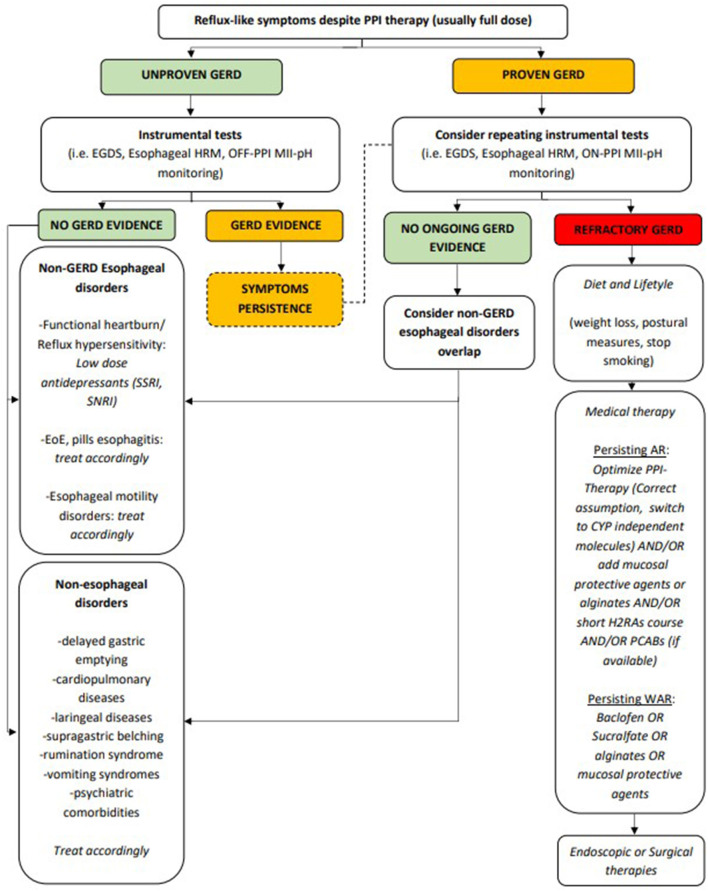
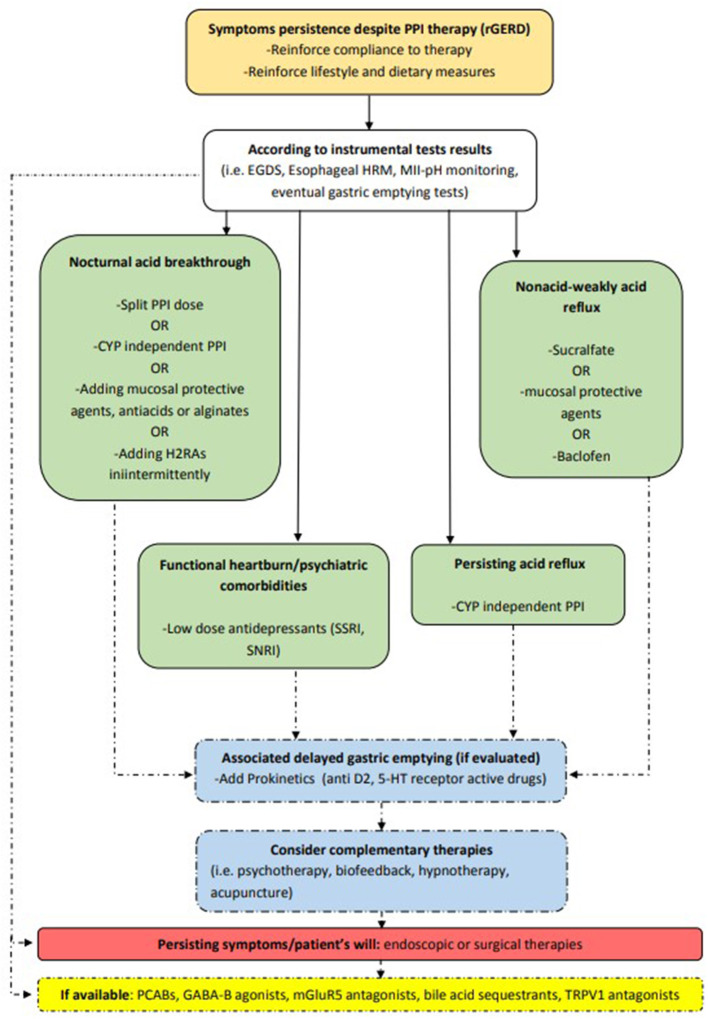
Gastroesophageal reflux disease (GERD) is one of the most frequent gastrointestinal disorders. Proton pump inhibitors (PPIs) are effective in healing lesions and improving symptoms in most cases, although up to 40% of GERD patients do not respond adequately to PPI therapy. Refractory GERD (rGERD) is one of the most challenging problems, given its impact on the quality of life and consumption of health care resources. The definition of rGERD is a controversial topic as it has not been unequivocally established. Indeed, some patients unresponsive to PPIs who experience symptoms potentially related to GERD may not have GERD; in this case the definition could be replaced with "reflux-like PPI-refractory symptoms." Patients with persistent reflux-like symptoms should undergo a diagnostic workup aimed at finding objective evidence of GERD through endoscopic and pH-impedance investigations. The management strategies regarding rGERD, apart from a careful check of patient's compliance with PPIs, a possible change in the timing of their administration and the choice of a PPI with a different metabolic pathway, include other pharmacologic treatments. These include histamine-2 receptor antagonists (H2RAs), alginates, antacids and mucosal protective agents, potassium competitive acid blockers (PCABs), prokinetics, gamma aminobutyric acid-B (GABA-B) receptor agonists and metabotropic glutamate receptor-5 (mGluR5) antagonists, and pain modulators. If there is no benefit from medical therapy, but there is objective evidence of GERD, invasive antireflux options should be evaluated after having carefully explained the risks and benefits to the patient. The most widely performed invasive antireflux option remains laparoscopic antireflux surgery (LARS), even if other, less invasive, interventions have been suggested in the last few decades, including endoscopic transoral incisionless fundoplication (TIF), magnetic sphincter augmentation (LINX) or radiofrequency therapy (Stretta). Due to the different mechanisms underlying rGERD, the most effective strategy can vary, and it should be tailored to each patient. The aim of this paper is to review the different management options available to successfully deal with rGERD.
Keywords: 24-h multichannel intraluminal impedance-pH (MII-pH); gastroesophageal reflux disease (GERD); laparoscopic antireflux surgery (LARS); proton pump inhibitors (PPIs); refractory GERD (rGERD).
Copyright © 2021 Rettura, Bronzini, Campigotto, Lambiase, Pancetti, Berti, Marchi, de Bortoli, Zerbib, Savarino and Bellini.
Conflict of interest statement
FZ was employed by company CHU de Bordeaux. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- Sigterman KE, van Pinxteren B, Bonis PA, Lau J, Numans ME. Short-term treatment with proton pump inhibitors, H2-receptor antagonists and prokinetics for gastro-oesophageal reflux disease-like symptoms and endoscopy negative reflux disease. Cochrane Database Syst Rev. (2013) 2013:CD002095. 10.1002/14651858.CD002095.pub5 - DOI - PMC - PubMed
Publication types
LinkOut - more resources
Full Text Sources