

Natriuresis-guided therapy in acute heart failure: rationale and design of the Pragmatic Urinary Sodium-based treatment algoritHm in Acute Heart Failure (PUSH-AHF) trial
- PMID: 34791756
- PMCID: PMC9306663
- DOI: 10.1002/ejhf.2385
Natriuresis-guided therapy in acute heart failure: rationale and design of the Pragmatic Urinary Sodium-based treatment algoritHm in Acute Heart Failure (PUSH-AHF) trial
Abstract
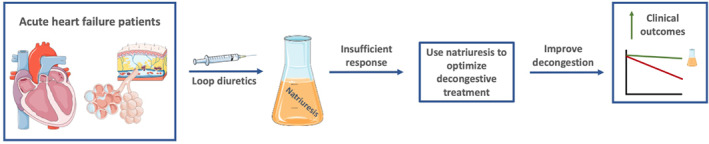
Aims: Insufficient diuretic response frequently occurs in patients admitted for acute heart failure (HF) and is associated with worse clinical outcomes. Recent studies have shown that measuring natriuresis early after hospital admission could reliably identify patients with a poor diuretic response during hospitalization who might require enhanced diuretic treatment. This study will test the hypothesis that natriuresis-guided therapy in patients with acute HF improves natriuresis and clinical outcomes.
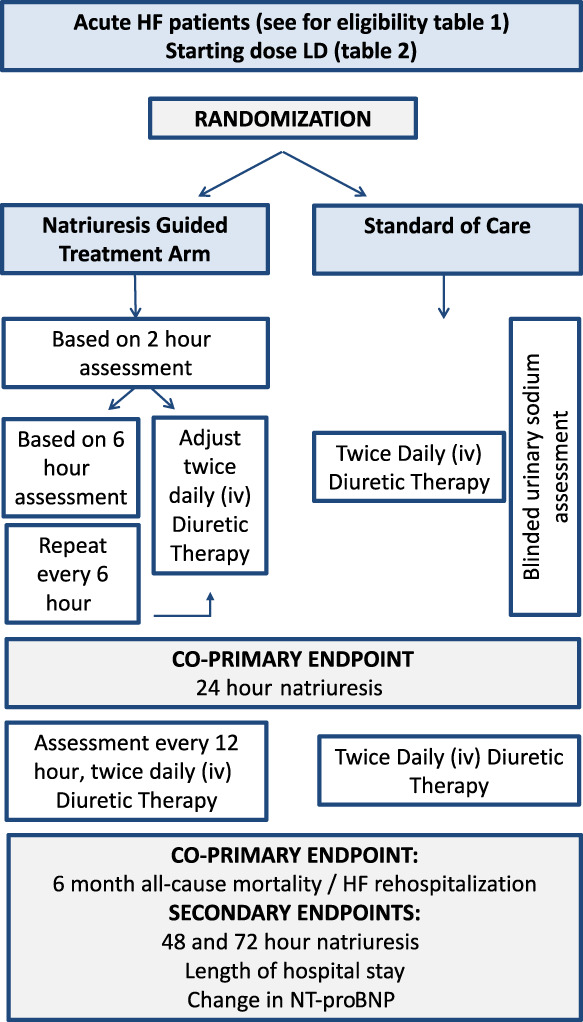
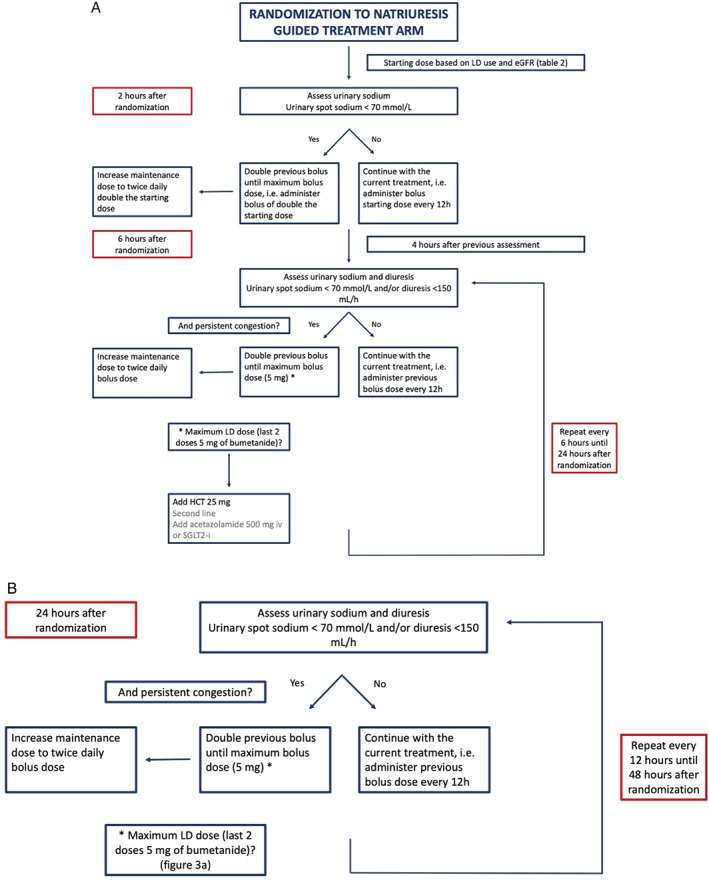
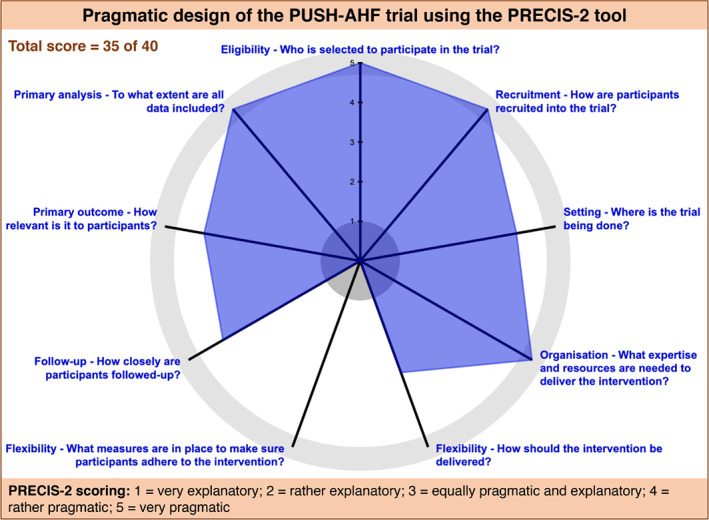
Methods: The Pragmatic Urinary Sodium-based treatment algoritHm in Acute Heart Failure (PUSH-AHF) is a pragmatic, single-centre, randomized, controlled, open-label study, aiming to recruit 310 acute HF patients requiring treatment with intravenous loop diuretics. Patients will be randomized to natriuresis-guided therapy or standard of care. Natriuresis will be determined at set time points after initiation of intravenous loop diuretics, and treatment will be adjusted based on the urinary sodium levels in the natriuresis-guided group using a pre-specified stepwise approach of increasing doses of loop diuretics and the initiation of combination diuretic therapy. The co-primary endpoint is 24-h urinary sodium excretion after start of loop diuretic therapy and a combined endpoint of all-cause mortality or first HF rehospitalization at 6 months. Secondary endpoints include 48- and 72-h sodium excretion, length of hospital stay, and percentage change in N-terminal pro brain natriuretic peptide at 48 and 72 h.
Conclusion: The PUSH-AHF study will investigate whether natriuresis-guided therapy, using a pre-specified stepwise diuretic treatment approach, improves natriuresis and clinical outcomes in patients with acute HF.
© 2021 The Authors. European Journal of Heart Failure published by John Wiley & Sons Ltd on behalf of European Society of Cardiology.
Figures
References
-
- Gheorghiade M, Vaduganathan M, Fonarow GC, Bonow RO. Rehospitalization for heart failure: problems and perspectives. J Am Coll Cardiol. 2013;61:391–403. - PubMed
-
- Valente MA, Voors AA, Damman K, Van Veldhuisen DJ, Massie BM, O'Connor CM, et al. Diuretic response in acute heart failure: clinical characteristics and prognostic significance. Eur Heart J. 2014;35:1284–93. - PubMed
-
- ter Maaten JM, Valente MA, Damman K, Hillege HL, Navis G, Voors AA. Diuretic response in acute heart failure‐pathophysiology, evaluation, and therapy. Nat Rev Cardiol. 2015;12:184–92. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
