

Clinical management of cannabis withdrawal
- PMID: 34791767
- PMCID: PMC9110555
- DOI: 10.1111/add.15743
Clinical management of cannabis withdrawal
Abstract
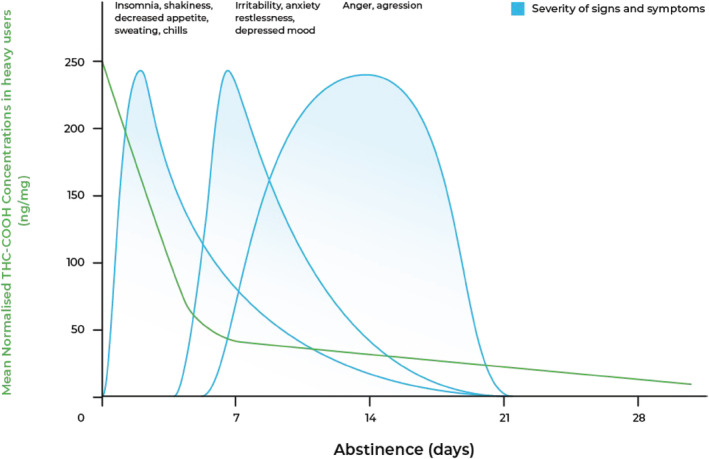
Background and aims: Cannabis withdrawal is a well-characterized phenomenon that occurs in approximately half of regular and dependent cannabis users after abrupt cessation or significant reductions in cannabis products that contain Δ9 -tetrahydrocannabinol (THC). This review describes the diagnosis, prevalence, course and management of cannabis withdrawal and highlights opportunities for future clinical research.
Methods: Narrative review of literature.
Results: Symptom onset typically occurs 24-48 hours after cessation and most symptoms generally peak at days 2-6, with some symptoms lasting up to 3 weeks or more in heavy cannabis users. The most common features of cannabis withdrawal are anxiety, irritability, anger or aggression, disturbed sleep/dreaming, depressed mood and loss of appetite. Less common physical symptoms include chills, headaches, physical tension, sweating and stomach pain. Despite limited empirical evidence, supportive counselling and psychoeducation are the first-line approaches in the management of cannabis withdrawal. There are no medications currently approved specifically for medically assisted withdrawal (MAW). Medications have been used to manage short-term symptoms (e.g. anxiety, sleep, nausea). A number of promising pharmacological agents have been examined in controlled trials, but these have been underpowered and positive findings not reliably replicated. Some (e.g. cannabis agonists) are used 'off-label' in clinical practice. Inpatient admission for MAW may be clinically indicated for patients who have significant comorbid mental health disorders and polysubstance use to avoid severe complications.
Conclusions: The clinical significance of cannabis withdrawal is that its symptoms may precipitate relapse to cannabis use. Complicated withdrawal may occur in people with concurrent mental health and polysubstance use.
Keywords: assessment; cannabis withdrawal syndrome; clinical management; pharmacology; prevalence; time course.
© 2021 The Authors. Addiction published by John Wiley & Sons Ltd on behalf of Society for the Study of Addiction.
Figures
References
-
- American Psychiatric Association . Diagnostic and Statistical Manual of Mental Disorders: DSM‐5. 5th ed. Washington, DC: American Psychiatric Association; 2013.
-
- Budney AJ, Hughes JR. The cannabis withdrawal syndrome. Curr Opin Psychiatry. 2006;19:233–8. - PubMed
-
- Taylor L, Crockett J, Tayo B, Checketts D, Sommerville K. Abrupt withdrawal of cannabidiol (CBD): a randomized trial. Epilepsy Behav. 2020;104:106938. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
