

Venetoclax in Previously Treated Waldenström Macroglobulinemia
- PMID: 34793256
- PMCID: PMC8683218
- DOI: 10.1200/JCO.21.01194
Venetoclax in Previously Treated Waldenström Macroglobulinemia
Abstract
Purpose: BCL2 is overexpressed and confers prosurvival signaling in malignant lymphoplasmacytic cells in Waldenström macroglobulinemia (WM). Venetoclax is a potent BCL2 antagonist and triggers in vitro apoptosis of WM cells. The activity of venetoclax in WM remains to be clarified.
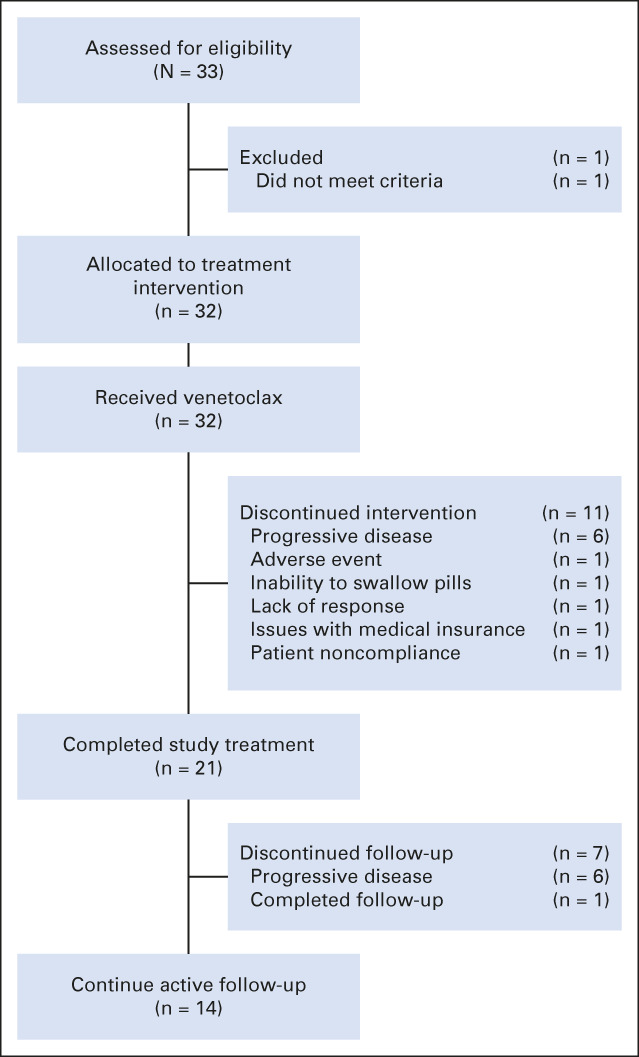
Patients and methods: We performed a multicenter, prospective phase II study of venetoclax in patients with previously treated WM (NCT02677324). Venetoclax was dose-escalated from 200 mg to a maximum dose of 800 mg daily for up to 2 years.
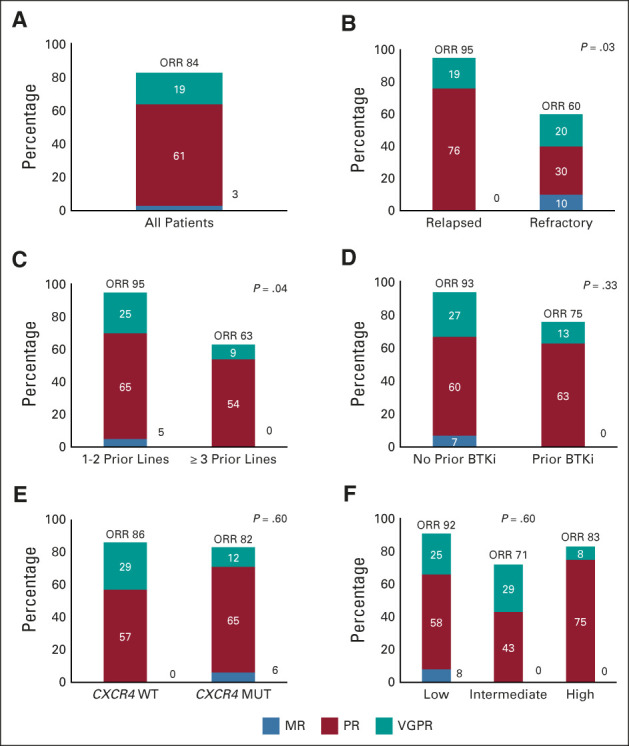
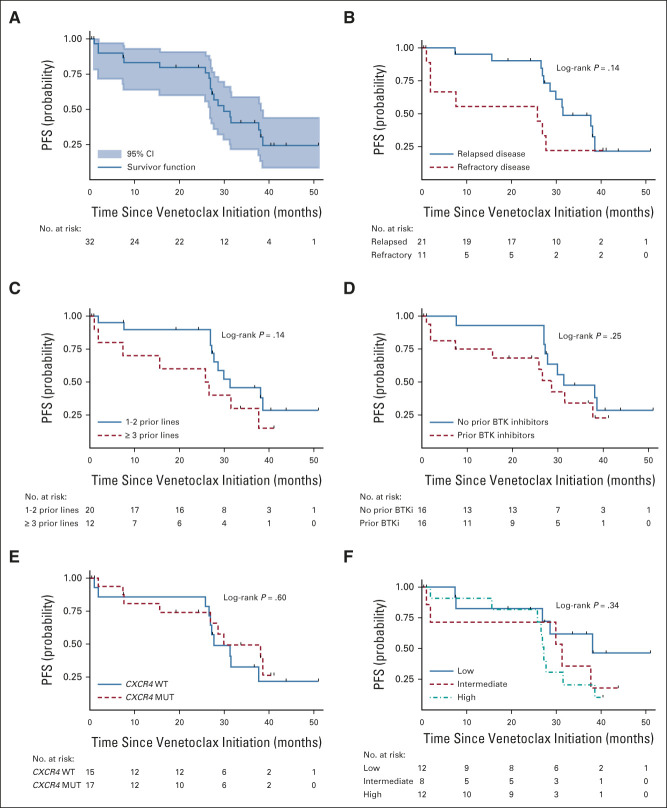
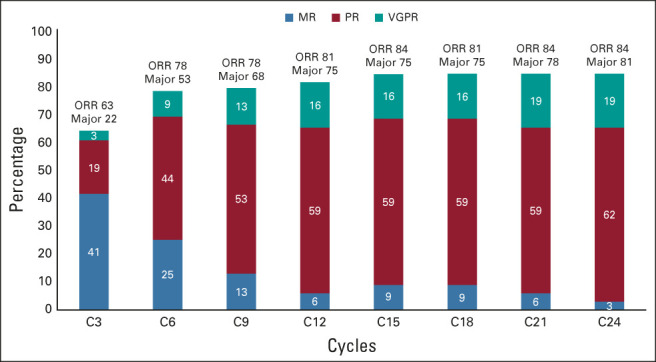
Results: Thirty-two patients were evaluable, including 16 previously exposed to Bruton tyrosine kinase inhibitors (BTKis). All patients were MYD88 L265P-mutated, and 17 carried CXCR4 mutations. The median time to minor and major responses was 1.9 and 5.1 months, respectively. Previous exposure to BTKis was associated with a longer time to response (4.5 v 1.4 months; P < .001). The overall, major, and very good partial response rates were 84%, 81%, and 19%, respectively. The major response rate was lower in those with refractory versus relapsed disease (50% v 95%; P = .007). The median follow-up time was 33 months, and the median progression-free survival was 30 months. CXCR4 mutations did not affect treatment response or progression-free survival. The only recurring grade ≥ 3 treatment-related adverse event was neutropenia (n = 14; 45%), including one episode of febrile neutropenia. Laboratory tumor lysis without clinical sequelae occurred in one patient. No deaths have occurred.
Conclusion: Venetoclax is safe and highly active in patients with previously treated WM, including those who previously received BTKis. CXCR4 mutation status did not affect treatment response.
Conflict of interest statement
Figures
References
-
- Owen RG, Treon SP, Al-Katib A, et al. : Clinicopathological definition of Waldenstrom's macroglobulinemia: Consensus panel recommendations from the Second International Workshop on Waldenstrom's Macroglobulinemia. Semin Oncol 30:110-115, 2003 - PubMed
-
- Castillo JJ, Advani RH, Branagan AR, et al. : Consensus treatment recommendations from the tenth International Workshop for Waldenstrom Macroglobulinaemia. Lancet Haematol 7:e827-e837, 2020 - PubMed
-
- Hunter ZR, Xu L, Yang G, et al. : The genomic landscape of Waldenstrom macroglobulinemia is characterized by highly recurring MYD88 and WHIM-like CXCR4 mutations, and small somatic deletions associated with B-cell lymphomagenesis. Blood 123:1637-1646, 2014 - PubMed
-
- Treon SP, Xu L, Yang G, et al. : MYD88 L265P somatic mutation in Waldenstrom's macroglobulinemia. N Engl J Med 367:826-833, 2012 - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
