

Development and validation of a prognostic tool: Pulmonary embolism short-term clinical outcomes risk estimation (PE-SCORE)
- PMID: 34793539
- PMCID: PMC8601564
- DOI: 10.1371/journal.pone.0260036
Development and validation of a prognostic tool: Pulmonary embolism short-term clinical outcomes risk estimation (PE-SCORE)
Abstract
Objective: Develop and validate a prognostic model for clinical deterioration or death within days of pulmonary embolism (PE) diagnosis using point-of-care criteria.
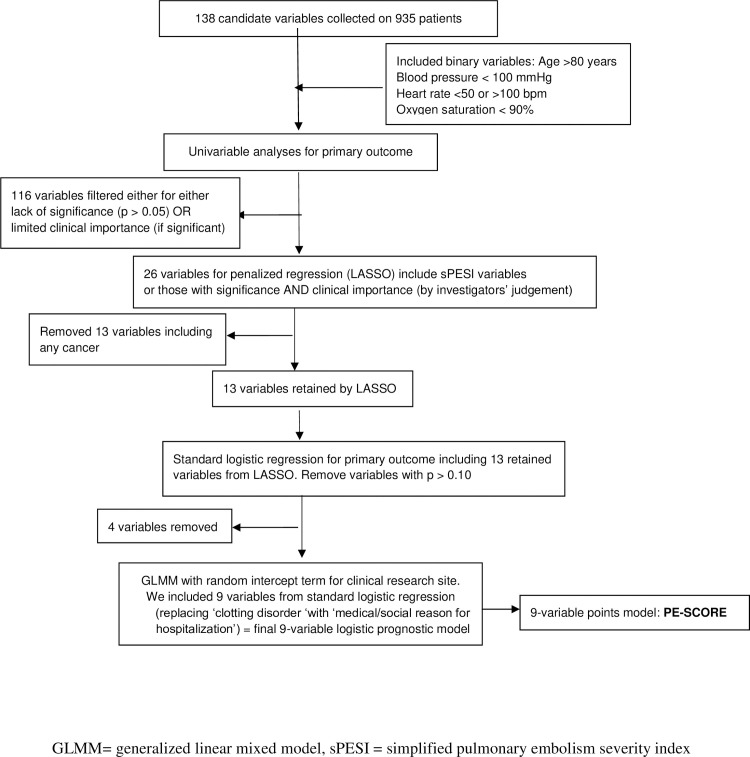
Methods: We used prospective registry data from six emergency departments. The primary composite outcome was death or deterioration (respiratory failure, cardiac arrest, new dysrhythmia, sustained hypotension, and rescue reperfusion intervention) within 5 days. Candidate predictors included laboratory and imaging right ventricle (RV) assessments. The prognostic model was developed from 935 PE patients. Univariable analysis of 138 candidate variables was followed by penalized and standard logistic regression on 26 retained variables, and then tested with a validation database (N = 801).
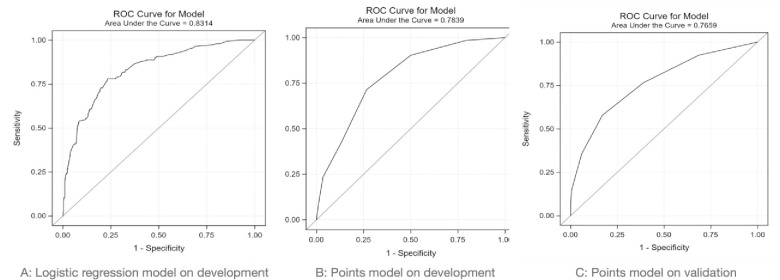
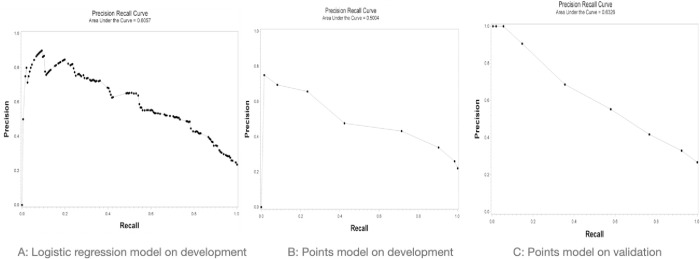
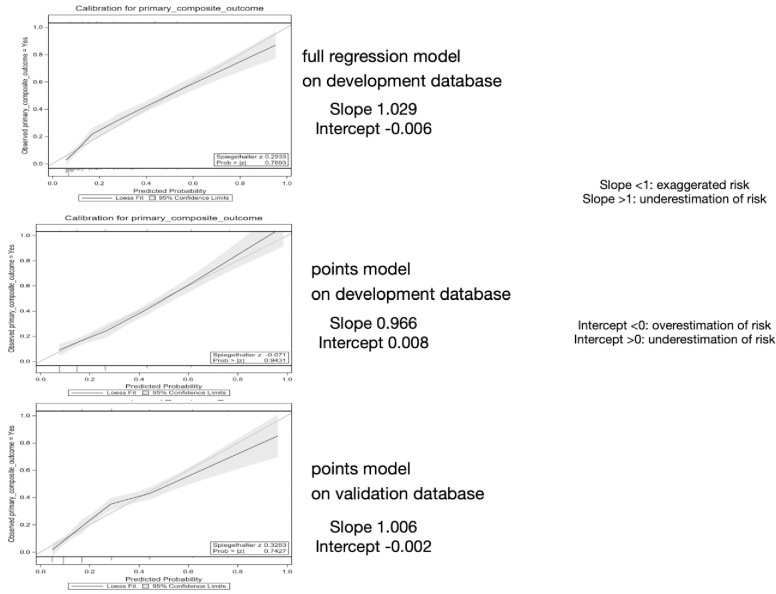
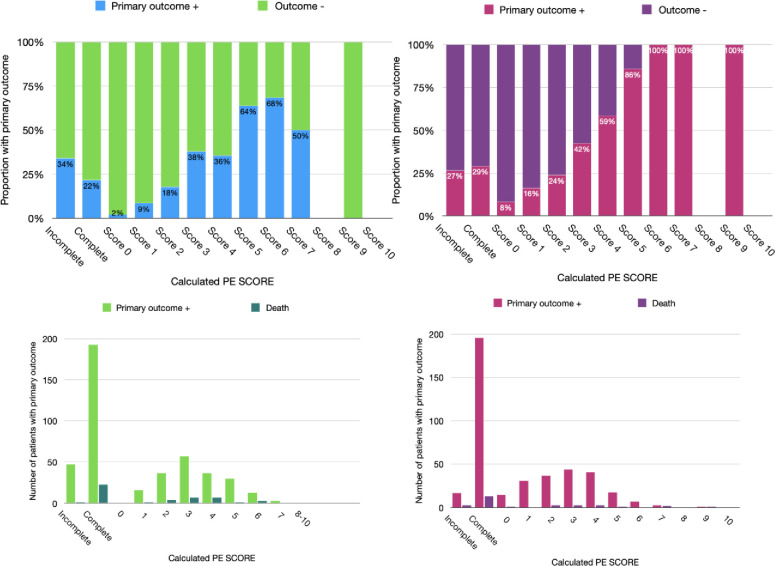
Results: Logistic regression yielded a nine-variable model, then simplified to a nine-point tool (PE-SCORE): one point each for abnormal RV by echocardiography, abnormal RV by computed tomography, systolic blood pressure < 100 mmHg, dysrhythmia, suspected/confirmed systemic infection, syncope, medico-social admission reason, abnormal heart rate, and two points for creatinine greater than 2.0 mg/dL. In the development database, 22.4% had the primary outcome. Prognostic accuracy of logistic regression model versus PE-SCORE model: 0.83 (0.80, 0.86) vs. 0.78 (0.75, 0.82) using area under the curve (AUC) and 0.61 (0.57, 0.64) vs. 0.50 (0.39, 0.60) using precision-recall curve (AUCpr). In the validation database, 26.6% had the primary outcome. PE-SCORE had AUC 0.77 (0.73, 0.81) and AUCpr 0.63 (0.43, 0.81). As points increased, outcome proportions increased: a score of zero had 2% outcome, whereas scores of six and above had ≥ 69.6% outcomes. In the validation dataset, PE-SCORE zero had 8% outcome [no deaths], whereas all patients with PE-SCORE of six and above had the primary outcome.
Conclusions: PE-SCORE model identifies PE patients at low- and high-risk for deterioration and may help guide decisions about early outpatient management versus need for hospital-based monitoring.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
