

SARS-CoV-2 exposure in Malawian blood donors: an analysis of seroprevalence and variant dynamics between January 2020 and July 2021
- PMID: 34794434
- PMCID: PMC8601780
- DOI: 10.1186/s12916-021-02187-y
SARS-CoV-2 exposure in Malawian blood donors: an analysis of seroprevalence and variant dynamics between January 2020 and July 2021
Abstract
Background: By August 2021, the COVID-19 pandemic has been less severe in sub-Saharan Africa than elsewhere. In Malawi, there have been three subsequent epidemic waves. We therefore aimed to describe the dynamics of SARS-CoV-2 exposure in Malawi.
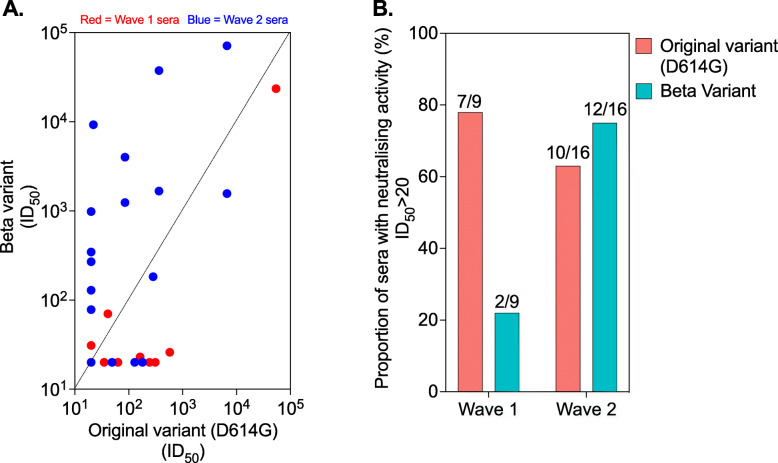
Methods: We measured the seroprevalence of anti-SARS-CoV-2 antibodies amongst randomly selected blood transfusion donor sera in Malawi from January 2020 to July 2021 using a cross-sectional study design. In a subset, we also assessed in vitro neutralisation against the original variant (D614G WT) and the Beta variant.
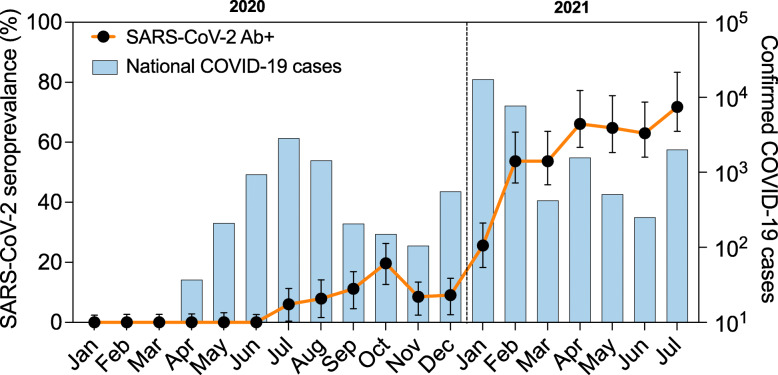
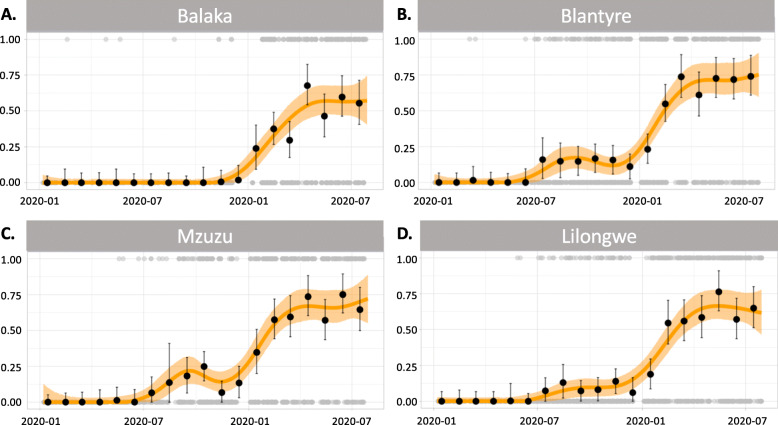
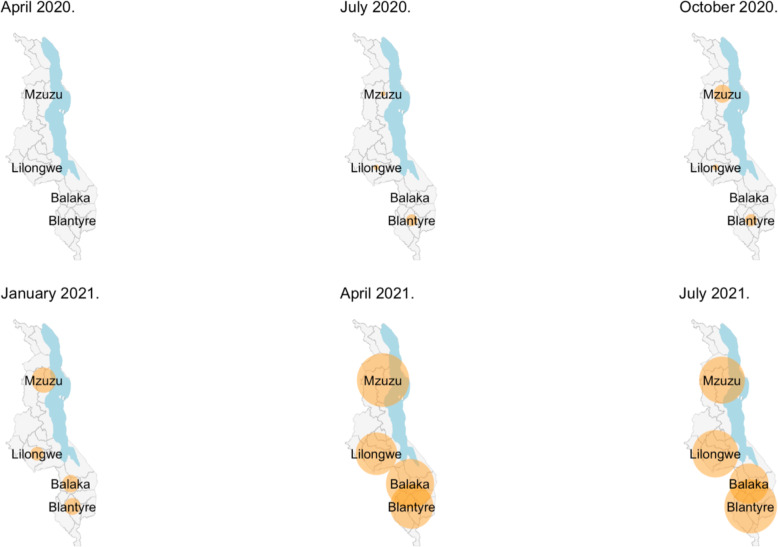
Results: A total of 5085 samples were selected from the blood donor database, of which 4075 (80.1%) were aged 20-49 years. Of the total, 1401 were seropositive. After adjustment for assay characteristics and applying population weights, seropositivity reached peaks in October 2020 (18.5%) and May 2021 (64.9%) reflecting the first two epidemic waves. Unlike the first wave, both urban and rural areas had high seropositivity in the second wave, Balaka (rural, 66.2%, April 2021), Blantyre (urban, 75.6%, May 2021), Lilongwe (urban, 78.0%, May 2021), and Mzuzu (urban, 74.6%, April 2021). Blantyre and Mzuzu also show indications of the start of a third pandemic wave with seroprevalence picking up again in July 2021 (Blantyre, 81.7%; Mzuzu, 71.0%). More first wave sera showed in vitro neutralisation activity against the original variant (78% [7/9]) than the beta variant (22% [2/9]), while more second wave sera showed neutralisation activity against the beta variant (75% [12/16]) than the original variant (63% [10/16]).
Conclusion: The findings confirm extensive SARS-CoV-2 exposure in Malawi over two epidemic waves with likely poor cross-protection to reinfection from the first on the second wave. The dynamics of SARS-CoV-2 exposure will therefore need to be taken into account in the formulation of the COVID-19 vaccination policy in Malawi and across the region. Future studies should use an adequate sample size for the assessment of neutralisation activity across a panel of SARS-CoV-2 variants of concern/interest to estimate community immunity.
Keywords: Blood donors; Malawi; SARS-CoV-2; Seroprevalence.
© 2021. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- COVID-19 case tracker [https://coronavirus.jhu.edu/map.html.]
-
- Walker PGT, Whittaker C, Watson OJ, Baguelin M, Winskill P, Hamlet A, Djafaara BA, Cucunubá Z, Olivera Mesa D, Green W, et al. The impact of COVID-19 and strategies for mitigation and suppression in low- and middle-income countries. Science. 2020;69(6502):413–422. doi: 10.1126/science.abc0035. - DOI - PMC - PubMed
-
- Morton B, Barnes KG, Anscombe C, Jere K, Matambo P, Mandolo J, Kamng’ona R, Brown C, Nyirenda J, Phiri T, et al. Distinct clinical and immunological profiles of patients with evidence of SARS-CoV-2 infection in sub-Saharan Africa. Nat Commun. 2021;12(1):3554. doi: 10.1038/s41467-021-23267-w. - DOI - PMC - PubMed
-
- Chibwana M, Jere K, Kamng’ona R, Mandolo J, Katunga-Phiri V, Tembo D, et al. High SARS-CoV-2 seroprevalence in health care workers but relatively low numbers of deaths in urban Malawi [version 2; peer review: 2 approved]. Wellcome Open Res. 2020;5(199):1–15.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
