

Analgesia in pediatric trauma patients in physician-staffed Austrian helicopter rescue: a 12-year registry analysis
- PMID: 34794486
- PMCID: PMC8600762
- DOI: 10.1186/s13049-021-00978-z
Analgesia in pediatric trauma patients in physician-staffed Austrian helicopter rescue: a 12-year registry analysis
Abstract
Background: As pediatric patients are typically rare among helicopter emergency medical systems (HEMS), children might be at risk for oligo-analgesia due to the rescuer's lack of experience and the fear of side effects.
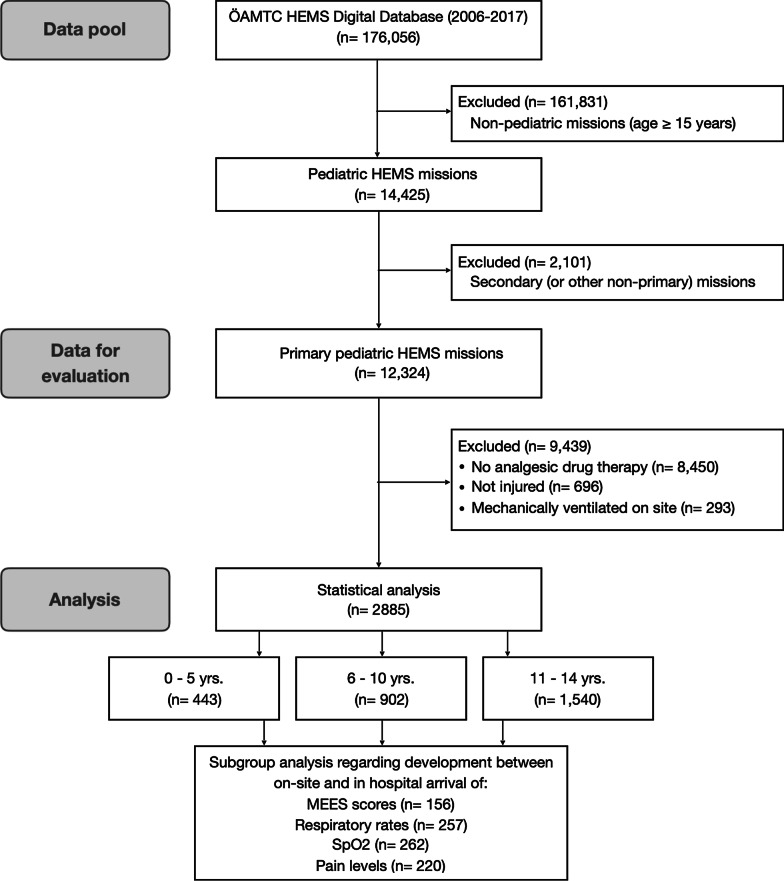
Methods: In this retrospective analysis, data was obtained from the ÖAMTC HEMS digital database including 14 physician staffed helicopter bases in Austria over a 12-year timeframe. Primary missions involving pediatric trauma patients (< 15 years) not mechanically ventilated on-site were included. Analgesia was assessed and compared between the age groups 0-5, 6-10 and 11-14 years.
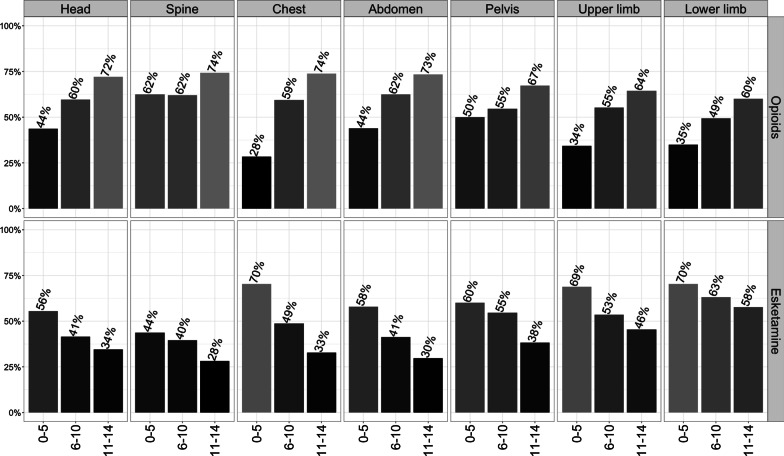
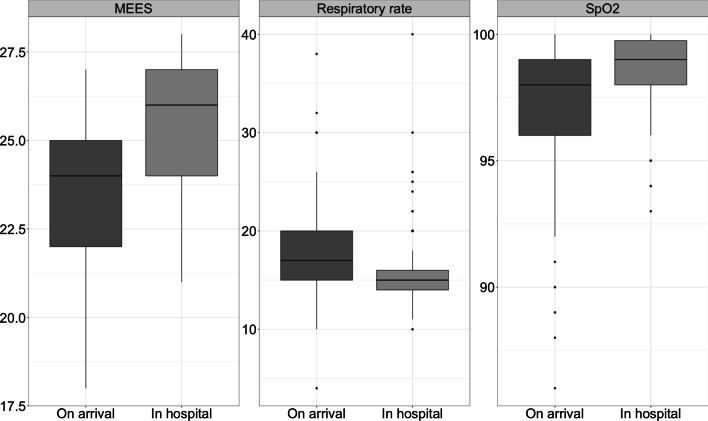
Results: Of all flight missions, 8.2% were dedicated to children < 15 years. Analgetic drugs were administered in 31.4% of all primary missions (3874 of 12,324), wherefrom 2885 were injured and non-ventilated (0-5 yrs.: n = 443; 6-10 yrs.: n = 902; 11-14 yrs.: n = 1540). The majority of these patients (> 75%) suffered moderate to severe pain, justifying immediate analgesia. HEMS physicians typically chose a monotherapy with an opioid (n = 1277; 44.3%) or Esketamine (n = 1187; 41.1%) followed by the combination of both (n = 324; 11.2%). Opioid use increased (37.2% to 63.4%) and Esketamine use decreased (66.1% to 48.3%) in children < 6 vs. > 10 years. Esketamine was more often administered in extremity (57.3%) than in head (41.5%) or spine injuries (32.3%). An intravenous access was less often established in children < 6 years (74.3% vs. 90.8%; p < 0.001). Despite the use of potent analgesics, 396 missions (13.7%) were performed without technical monitoring. Particularly regarding patient data at handover in hospital, merely < 10% of all missions featured complete documentation. Therefore, sufficient evaluation of the efficacy of pain relief was not possible. Yet, by means of respiratory measures required during transport, severe side effects such as respiratory insufficiency, were barely noted.
Conclusions: In the physician-staffed HEMS setting, pediatric trauma patients liberally receive opioids and Esketamine for analgesia. With regard to severe respiratory insufficiency during transport, the application of these potent analgesics seems safe.
Keywords: Accident; Air ambulance; Analgesia; Children; Emergency medicine services; Wounds and injuries.
© 2021. The Author(s).
Conflict of interest statement
None of the authors has competing interests regarding this manuscript.
Figures
References
-
- Scholten AC, Berben SAA, Westmaas AH, van Grunsven PM, de Vaal ET, Rood PPM, Hoogerwerf N, Doggen CJM, Schoonhoven L. Pain management in trauma patients in (pre)hospital based emergency care: current practice versus new guideline. Injury. 2015;46:798–806. doi: 10.1016/j.injury.2014.10.045. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
