

Immunogenicity and risk of Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) infection after Coronavirus Disease 2019 (COVID-19) vaccination in patients with cancer: a systematic review and meta-analysis
- PMID: 34794855
- PMCID: PMC8548030
- DOI: 10.1016/j.ejca.2021.10.014
Immunogenicity and risk of Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) infection after Coronavirus Disease 2019 (COVID-19) vaccination in patients with cancer: a systematic review and meta-analysis
Abstract
Background: Patients with cancer are considered a priority group for Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) vaccination given their high risk of contracting severe Coronavirus Disease 2019 (COVID-19). However, limited data exist regarding the efficacy of immunisation in this population. In this study, we assess the immunologic response after COVID-19 vaccination of cancer versus non-cancer population.
Methods: PubMed, Cochrane Central Register of Controlled Trials (CENTRAL), and Web of Science databases were searched from 01st March 2020 through 12th August 12 2021. Primary end-points were anti-SARS-CoV-2 spike protein (S) immunoglobulin G (IgG) seroconversion rates, T-cell response, and documented SARS-CoV-2 infection after COVID-19 immunisation. Data were extracted following the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) guidelines. Overall effects were pooled using random-effects models.
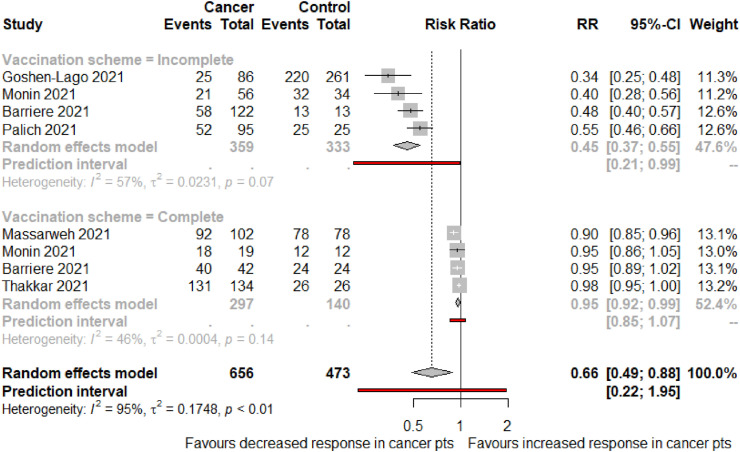
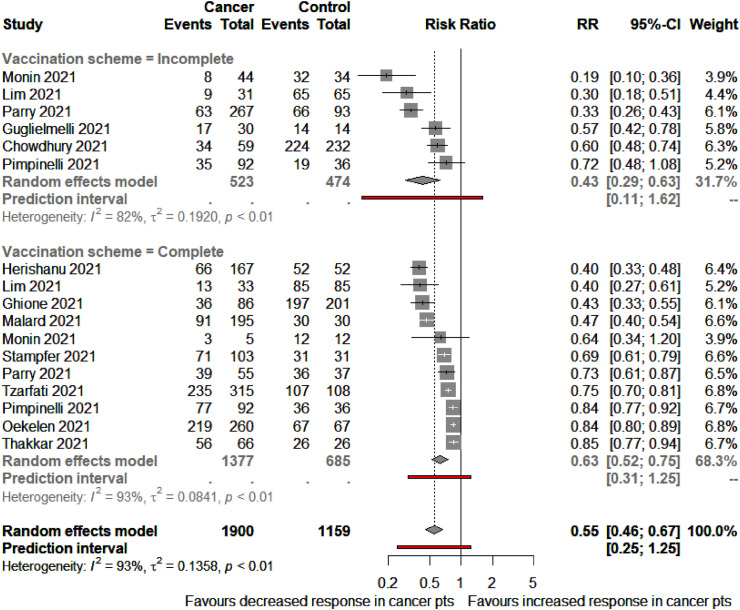
Results: This systematic review and meta-analysis included 35 original studies. Overall, 51% (95% confidence interval [CI], 41-62) and 73% (95% CI, 64-81) of patients with cancer developed anti-S IgG above the threshold level after partial and complete immunisation, respectively. Patients with haematologic malignancies had a significantly lower seroconversion rate than those with solid tumours after complete immunisation (65% vs 94%; P < 0.0001). Compared with non-cancer controls, oncological patients were less likely to attain seroconversion after incomplete (risk ratio [RR] 0.45 [95% CI 0.35-0.58]) and complete (RR 0.69 [95% CI 0.56-0.84]) COVID-19 immunisation schemes. Patients with cancer had a higher likelihood of having a documented SARS-CoV-2 infection after partial (RR 3.21; 95% CI 0.35-29.04) and complete (RR 2.04; 95% CI 0.38-11.10) immunisation.
Conclusions: Patients with cancer have an impaired immune response to COVID-19 vaccination compared with controls. Strategies that endorse the completion of vaccination schemes are warranted. Future studies should aim to evaluate different approaches that enhance oncological patients' immune response.
Keywords: COVID-19 breakthrough infections; COVID-19 vaccines; Haematologic neoplasms; Immunogenicity; Neoplasms; SARS-CoV-2; Vaccines.
Copyright © 2021 Elsevier Ltd. All rights reserved.
Figures






References
-
- Johns Hopkins Coronavirus Resource Center COVID-19 map - johns hopkins coronavirus resource center. https://coronavirus.jhu.edu/map.html
-
- Tagliamento M., Agostinetto E., Bruzzone M., Ceppi M., Saini K.S., de Azambuja E., et al. Mortality in adult patients with solid or hematological malignancies and SARS-CoV-2 infection with a specific focus on lung and breast cancers: a systematic review and meta-analysis. Crit Rev Oncol Hematol. 2021:163. doi: 10.1016/j.critrevonc.2021.103365. - DOI - PMC - PubMed
-
- WHO . 2021. WHO Director-General’s opening remarks at the media briefing on COVID-19 - 3 March 2020.https://www.who.int/director-general/speeches/detail/who-director-genera...
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
