

Transcranial Doppler Velocities and Angiographic Vasospasm after SAH: A Diagnostic Accuracy Study
- PMID: 34794947
- PMCID: PMC8757545
- DOI: 10.3174/ajnr.A7347
Transcranial Doppler Velocities and Angiographic Vasospasm after SAH: A Diagnostic Accuracy Study
Abstract
Background and purpose: After aneurysmal SAH, transcranial Doppler is commonly used to monitor cerebral vasospasm. The diagnostic accuracy of transcranial Doppler flow velocity values in detecting angiographic vasospasm in patients requiring urgent endovascular intervention has not been established.
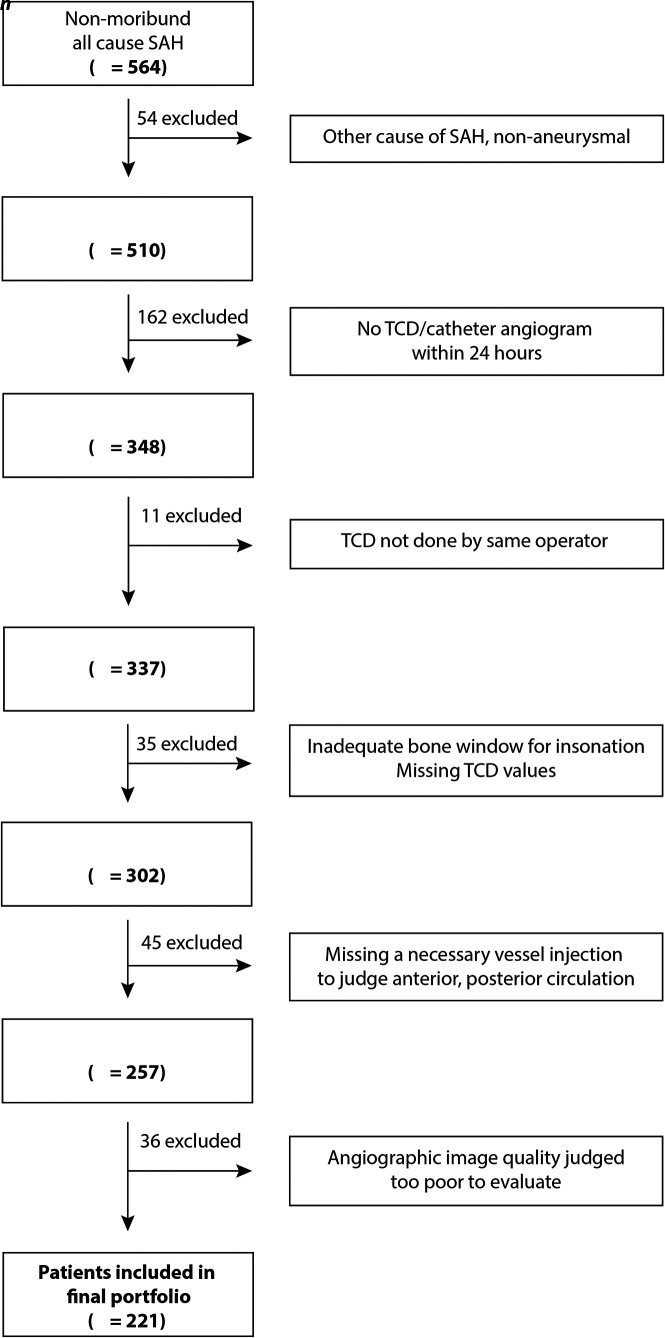
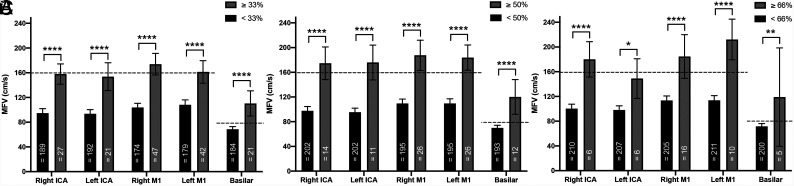
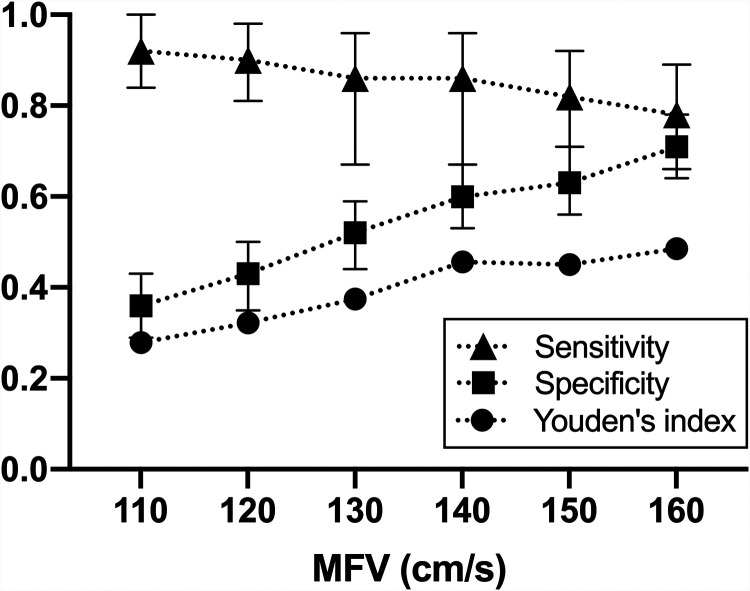
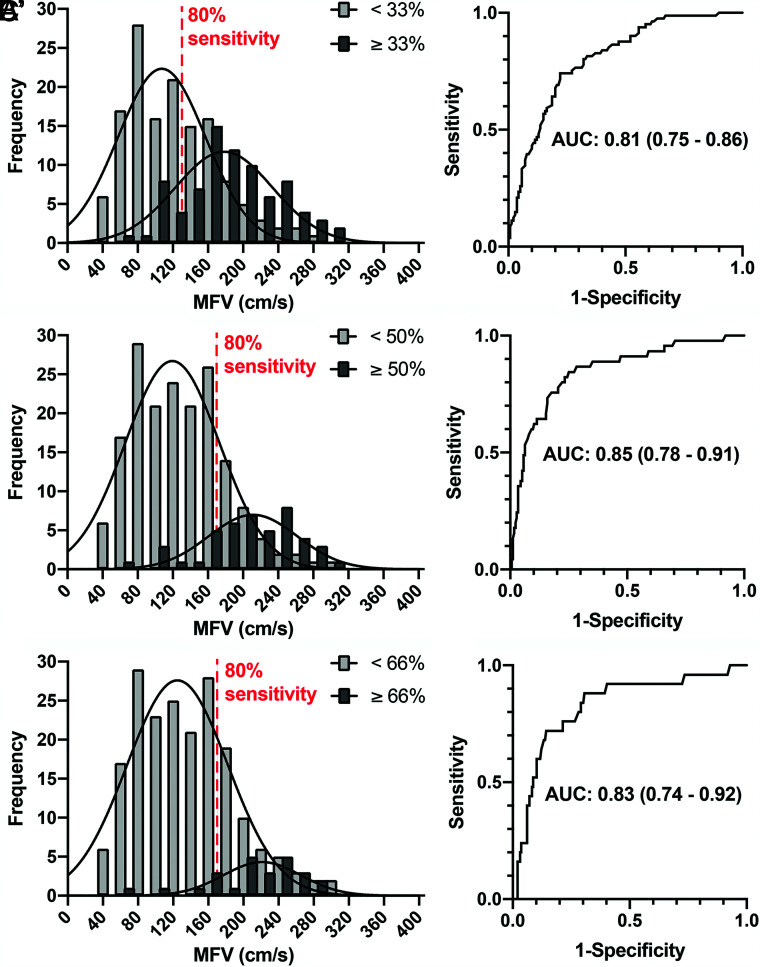
Materials and methods: We performed a retrospective analysis of a consecutive series of patients with aneurysmal SAH who underwent transcranial Doppler (index test) within 24 hours of conventional angiography (reference test). The judgment of 33%, 50%, and 66% degree of vessel narrowing on angiography was independently established by multiple neuroendovascular clinicians. Vessel-specific per-segment and per-patient transcranial Doppler velocities were studied using receiver operating characteristic curves, the Youden index, and minimal acceptable sensitivity models. Optimal mean flow-velocity thresholds were explored to calculate sensitivity and specificity using a per-patient judgment of vasospasm of at least 50% angiographic narrowing in any large arterial segment except A1.
Results: In 221 patients, vasospasm was found in 15%, 8%, and 4% of arteries when the degree of reference angiographic luminal narrowing was 33%, 50%, and 66%, respectively. Mean flow velocities were significantly higher in vasospastic segments (P = . 001), but per-segment exploratory analyses yielded unsound mean flow velocity thresholds. The Youden and minimal acceptable sensitivity models proposed mean flow velocity thresholds of approximately 160 cm/s for the anterior circulation and 80 cm/s for the posterior circulation in the per-patient diagnosis of angiographic vasospasm (≥50%), yielding a sensitivity of 80%-90% (95% CI, 0.77-0.96), but with a corresponding specificity of 50% (95% CI, 0.40-0.56).
Conclusions: In this study, a threshold transcranial Doppler mean flow-velocity value that would accurately diagnose ≥50% angiographic vasospasm remained elusive.
© 2022 by American Journal of Neuroradiology.
Figures
Comment in
-
Reply.AJNR Am J Neuroradiol. 2022 Mar;43(3):E4. doi: 10.3174/ajnr.A7454. Epub 2022 Mar 3. AJNR Am J Neuroradiol. 2022. PMID: 35241423 Free PMC article. No abstract available.
-
The Complementary Role of CT Perfusion and Transcranial Doppler in the Assessment of Delayed Cerebral Ischemia after Aneurysmal SAH.AJNR Am J Neuroradiol. 2022 Mar;43(3):E3. doi: 10.3174/ajnr.A7417. Epub 2022 Mar 3. AJNR Am J Neuroradiol. 2022. PMID: 35241424 Free PMC article. No abstract available.
References
-
- Gonzalez NR, Boscardin WJ, Glenn T, et al. . Vasospasm probability index: a combination of transcranial Doppler velocities, cerebral blood flow, and clinical risk factors to predict cerebral vasospasm after aneurysmal subarachnoid hemorrhage. J Neurosurg 2007;107:1101–12 10.3171/JNS-07/12/1101 - DOI - PubMed
-
- Lindegaard KF, Nornes H, Bakke SJ, et al. . Cerebral vasospasm after subarachnoid haemorrhage investigated by means of transcranial Doppler ultrasound. Acta Neurochir Suppl (Wien) 1988;42:81–84 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources