

Stratification of the risk of developing severe or lethal Covid-19 using a new score from a large Italian population: a population-based cohort study
- PMID: 34794995
- PMCID: PMC8602929
- DOI: 10.1136/bmjopen-2021-053281
Stratification of the risk of developing severe or lethal Covid-19 using a new score from a large Italian population: a population-based cohort study
Abstract
Objectives: To develop a population-based risk stratification model (COVID-19 Vulnerability Score) for predicting severe/fatal clinical manifestations of SARS-CoV-2 infection, using the multiple source information provided by the healthcare utilisation databases of the Italian National Health Service.
Design: Retrospective observational cohort study.
Setting: Population-based study using the healthcare utilisation database from five Italian regions.
Participants: Beneficiaries of the National Health Service, aged 18-79 years, who had the residentship in the five participating regions. Residents in a nursing home were not included. The model was built from the 7 655 502 residents of Lombardy region.
Main outcome measure: The score included gender, age and 29 conditions/diseases selected from a list of 61 conditions which independently predicted the primary outcome, that is, severe (intensive care unit admission) or fatal manifestation of COVID-19 experienced during the first epidemic wave (until June 2020). The score performance was validated by applying the model to several validation sets, that is, Lombardy population (second epidemic wave), and the other four Italian regions (entire 2020) for a total of about 15.4 million individuals and 7031 outcomes. Predictive performance was assessed by discrimination (areas under the receiver operating characteristic curve) and calibration (plot of observed vs predicted outcomes).
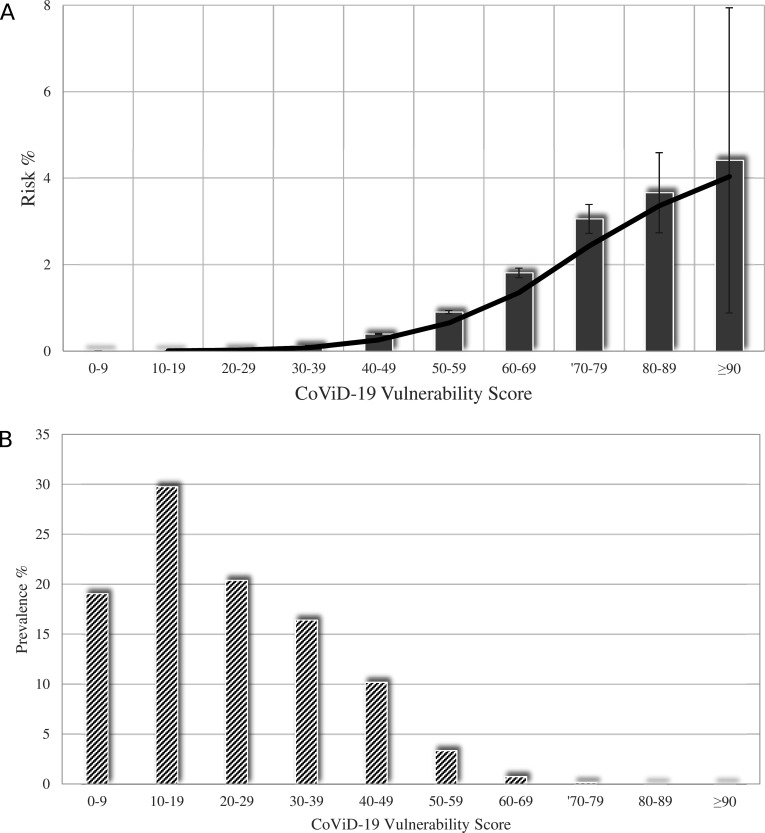
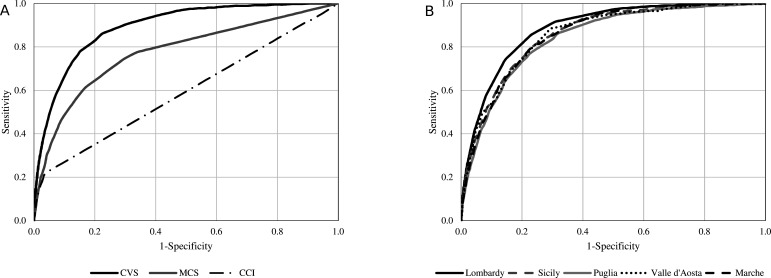
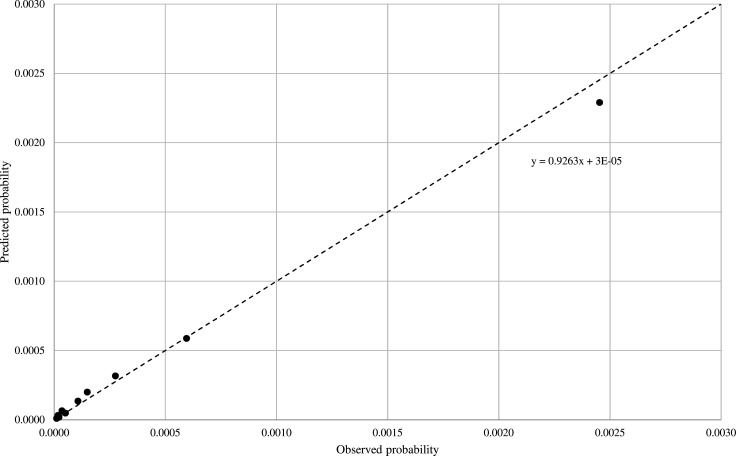
Results: We observed a clear positive trend towards increasing outcome incidence as the score increased. The areas under the receiver operating characteristic curve of the COVID-19 Vulnerability Score ranged from 0.85 to 0.88, which compared favourably with the areas of generic scores such as the Charlson Comorbidity Score (0.60). A remarkable performance of the score on the calibration of observed and predicted outcome probability was also observed.
Conclusions: A score based on data used for public health management accurately predicted the occurrence of severe/fatal manifestations of COVID-19. Use of this score may help health decision-makers to more accurately identify high-risk citizens who need early preventive or treatment interventions.
Keywords: COVID-19; health policy; public health.
© Author(s) (or their employer(s)) 2021. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: GC received research support from the European Community (EC), the Italian Agency of Drug (AIFA), the Italian Ministry of Education, University and Research (MIUR), and the Italian Health Ministry. He took part in a variety of projects that were funded by pharmaceutical companies (ie, Novartis, GSK, Roche, AMGEN and BMS). He also received honoraria as member of Advisory Board from Roche. GM received honoraria for participation as speaker/chairman in national/international meetings from Boehringer Ingelheim, Ferrer, Medtronic, Menarini, Merck Serono, Recordati and Servier.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous