

Comparison of two strategies for managing in-hospital cardiac arrest
- PMID: 34795366
- PMCID: PMC8602649
- DOI: 10.1038/s41598-021-02027-2
Comparison of two strategies for managing in-hospital cardiac arrest
Abstract
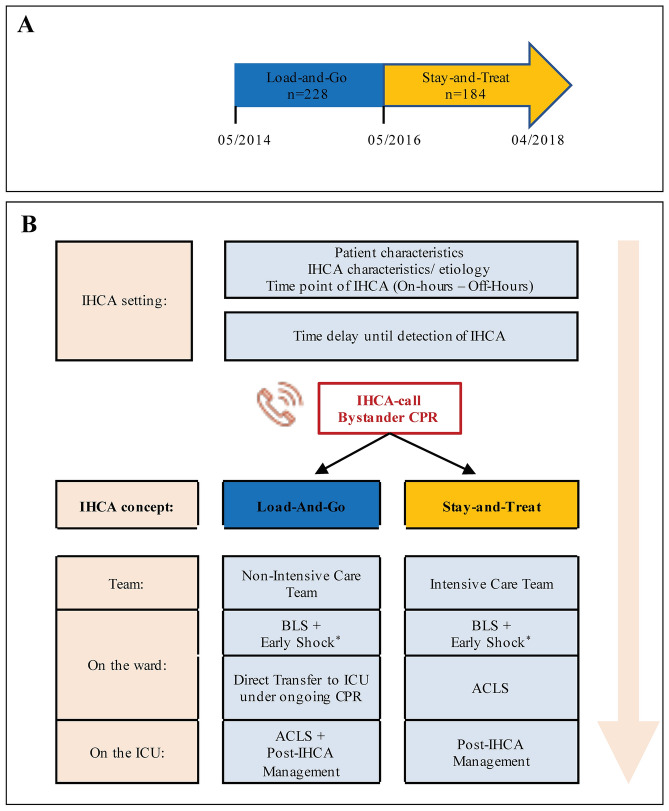
In-hospital cardiac arrest (IHCA) is associated with poor outcomes. There are currently no standards for cardiac arrest teams in terms of member composition and task allocation. Here we aimed to compare two different cardiac arrest team concepts to cover IHCA management in terms of survival and neurological outcomes. This prospective study enrolled 412 patients with IHCA from general medical wards. From May 2014 to April 2016, 228 patients were directly transferred to the intensive care unit (ICU) for ongoing resuscitation. In the ICU, resuscitation was extended to advanced cardiac life support (ACLS) (Load-and-Go [LaG] group). By May 2016, a dedicated cardiac arrest team provided by the ICU provided ACLS in the ward. After return of spontaneous circulation (ROSC), the patients (n = 184) were transferred to the ICU (Stay-and-Treat [SaT] group). Overall, baseline characteristics, aetiologies, and characteristics of cardiac arrest were similar between groups. The time to endotracheal intubation was longer in the LaG group than in the SaT group (6 [5, 8] min versus 4 [2, 5] min, p = 0.001). In the LaG group, 96% of the patients were transferred to the ICU regardless of ROSC achievement. In the SaT group, 83% of patients were transferred to the ICU (p = 0.001). Survival to discharge did not differ between the LaG (33%) and the SaT (35%) groups (p = 0.758). Ultimately, 22% of patients in the LaG group versus 21% in the SaT group were discharged with good neurological outcomes (p = 0.857). In conclusion, we demonstrated that the cardiac arrest team concepts for the management of IHCA did not differ in terms of survival and neurological outcomes. However, a dedicated (intensive care) cardiac arrest team could take some load off the ICU.
© 2021. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures

Similar articles
-
Location of In-Hospital Cardiac Arrest in the United States-Variability in Event Rate and Outcomes.J Am Heart Assoc. 2016 Sep 29;5(10):e003638. doi: 10.1161/JAHA.116.003638. J Am Heart Assoc. 2016. PMID: 27688235 Free PMC article.
-
Outcomes of in-hospital cardiac arrest managed with and without a specialized code team: A retrospective observational study.PLoS One. 2024 Sep 20;19(9):e0309376. doi: 10.1371/journal.pone.0309376. eCollection 2024. PLoS One. 2024. PMID: 39302946 Free PMC article.
-
The effect of adherence to ACLS protocols on survival of event in the setting of in-hospital cardiac arrest.Resuscitation. 2014 Jan;85(1):82-7. doi: 10.1016/j.resuscitation.2013.09.019. Epub 2013 Oct 5. Resuscitation. 2014. PMID: 24103233 Free PMC article.
-
[Managing the post-cardiac arrest syndrome. Directing Committee of the National Cardiopulmonary Resuscitation Plan (PNRCP) of the Spanish Society for Intensive Medicine, Critical Care and Coronary Units (SEMICYUC)].Med Intensiva. 2010 Mar;34(2):107-26. doi: 10.1016/j.medin.2009.09.001. Epub 2009 Nov 22. Med Intensiva. 2010. PMID: 19931943 Spanish.
-
Trends in In-Hospital Cardiac Arrest and Mortality Among Children With Cardiac Disease in the Intensive Care Unit: A Systematic Review and Meta-analysis.JAMA Netw Open. 2023 Feb 1;6(2):e2256178. doi: 10.1001/jamanetworkopen.2022.56178. JAMA Netw Open. 2023. PMID: 36763356 Free PMC article.
Cited by
-
Elevated Initial Serum Phosphate Levels Predict Higher Mortality and Impaired Neurological Outcome in Cardiac Arrest Patients with Return of Spontaneous Circulation.Diagnostics (Basel). 2023 Jan 28;13(3):479. doi: 10.3390/diagnostics13030479. Diagnostics (Basel). 2023. PMID: 36766585 Free PMC article.
-
Reduced mobility is associated with adverse outcomes after in-hospital cardiac arrest.Rev Assoc Med Bras (1992). 2023 Oct 30;69(12):e20230947. doi: 10.1590/1806-9282.20230947. eCollection 2023. Rev Assoc Med Bras (1992). 2023. PMID: 37909534 Free PMC article.
-
Roles of anesthesia assistants within the code blue team at in-hospital cardiopulmonary arrests: A retrospective analysis.Can J Respir Ther. 2025 Apr 25;61:78-86. doi: 10.29390/001c.136463. eCollection 2025. Can J Respir Ther. 2025. PMID: 40291484 Free PMC article.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
