

Periostin as a Biomarker of Allergic Inflammation in Atopic Bronchial Asthma and Allergic Rhinitis (a Pilot Study)
- PMID: 34796003
- PMCID: PMC8596267
- DOI: 10.17691/stm2020.12.5.04
Periostin as a Biomarker of Allergic Inflammation in Atopic Bronchial Asthma and Allergic Rhinitis (a Pilot Study)
Abstract
The involvement of periostin in Th2-dependent allergic inflammation has been documented. However, the significance of periostin as a biomarker of local allergic inflammation in the nasal mucosa (NM) of patients with atopic bronchial asthma (BA) and allergic rhinitis (AR) is yet to be determined. The aim of the study was to determine the presence of periostin and evaluate its role as a non-invasive marker of allergic inflammation in the nasal secretions of children with atopic BA and AR.
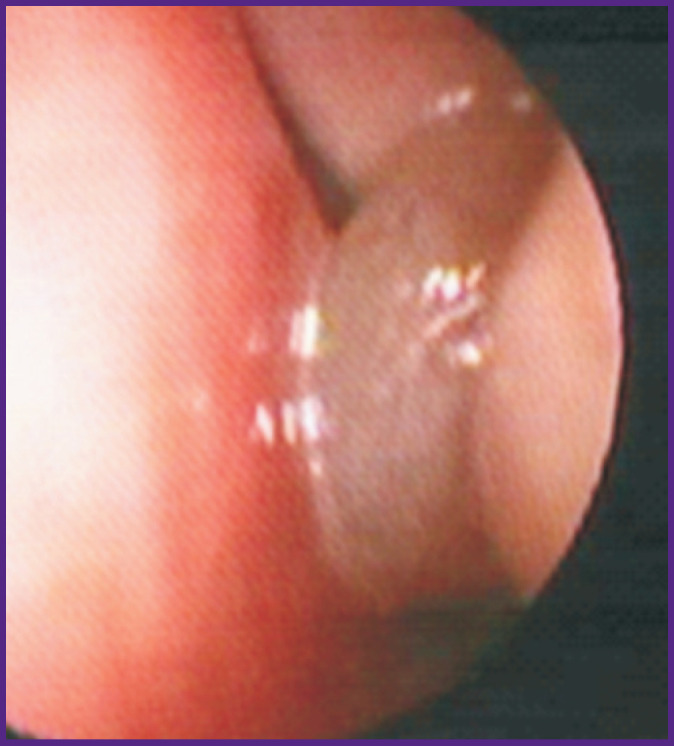
Materials and methods: In 43 patients aged 4-17 years with atopic BA and AR, the NM was examined using nasal video-endoscopy and (if indicated) computed tomography; the amount of periostin in the nasal secretion was determined by the enzyme immunoassay.
Results: Exacerbation of AR was accompanied by a statistically significant increase in the level of periostin in the nasal secretion: up to 0.84 [0.06; 48.79] ng/mg, whereas in remission, that was 0.13 [0.00; 0.36] ng/mg; p=0.04. This value increased progressively as the severity of AR increased from 0.16 [0.00; 0.36] ng/mg in the mild course to 0.20 [0.00; 9.03] ng/mg in AR of moderate severity, and to 10.70 [0.56; 769.20] ng/mg in most severe cases; p=0.048. Hypertrophy or polyposis of the nasal and/or paranasal mucosa was detected in 34.9% (15/43) of the examined patients. The concentration of periostin in the nasal secretion was lower in children without NM hypertrophy: 0.18 [0.001; 4.30] ng/mg vs 0.78 [0.13; 162.10] ng/mg in patients with NM hypertrophy; the differences were close to statistically significant: p=0.051. The level of nasal periostin depended on the clinical form of hypertrophy in the sinonasal mucosa, reaching 0.17 [0.00; 0.32] ng/mg in children with polyposis hyperplasia of NM and 21.6 [10.70; 1516.80] ng/mg - with hypertrophy of the NM in the medial surface of the concha; p=0.02.
Conclusion: Exacerbation and increased severity of AR in patients with atopic BA are accompanied by an increased level of periostin in the nasal secretion. This allows us to consider the level of nasal periostin as a biomarker of local allergic inflammation in the NM of patients with atopic BA combined with AR. Hypertrophic changes in the sinonasal mucosa are generally accompanied by an increased level of nasal periostin; specifically, this level significantly depends on the clinical form of mucous membrane hypertrophy and requires additional studies.
Keywords: allergic rhinitis; bronchial asthma; chronic rhinosinusitis with polyps; periostin.
Conflict of interest statement
Conflict of interest. The authors have confirmed that there are no obvious and potential conflicts of interest that need to be reported.
Figures

References
-
- GINA. Global strategy for asthma management and prevention. 2019 URL: https://ginasthma.org/wp-content/up-loads/2019/06/GINA-2019-main-report-...
-
- Reddel H.K., FitzGerald J.M., Bateman E.D., Bacharier L.B., Becker A., Brusselle G., Buhl R., Cruz A.A., Fleming L., Inoue H., Ko F.W., Krishnan J.A., Levy M.L., Lin J., Pedersen S.E., Sheikh A., Yorgancioglu A., Boulet L.P. GINA 2019: a fundamental change in asthma management: treatment of asthma with short-acting bronchodilators alone is no longer recommended for adults and adolescents. Eur Respir J. 2019;53(6):1901046. doi: 10.1183/13993003.01046-2019. - DOI - PubMed
-
- Krasilnikova S.V., Eliseeva T.I., Popov K.S., Tush E.V., Khaletskaya O.V., Ovsyannikov D.Y., Balabolkin I.I., Shakhov A.V., Prahov A.V. Multimorbidity of upper respiratory tract pathology in children with bronchial asthma. Pediatria. Zhurnal im. G.N. Speranskogo. 2018;97(2):19–26.
-
- Krasilnikova S.V., Eliseeva Т.I., Shakhov А.V., Geppe N.A. Capabilities of nasal videoendoscopy in diagnostics of pharyngeal tonsil condition in children with bronchial asthma. Sovremennye tehnologii v medicine. 2016;8(3):126–136. doi: 10.17691/stm2016.8.3.15. - DOI
-
- Krasilnikova S.V., Tush Е.V., Babaev S.Yu., Khaletskaya A.I., Popov K.S., Novozhilov A.A., Abubakirov T.E., Eliseeva Т.I., Ignatov S.K., Shakhov A.V., Kubysheva N.I., Solovyev V.D. Endonasal infrared thermometry for the diagnosis of allergic inflammation of the nasal mucosa in patients with bronchial asthma. Sovremennye tehnologii v medicine. 2017;9(4):201–208. doi: 10.17691/stm2017.9.4.25. - DOI
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials