Optimal First-Line Antibiotic Treatment for Pediatric Complicated Appendicitis Based on Peritoneal Fluid Culture
- PMID: 34796095
- PMCID: PMC8593360
- DOI: 10.5223/pghn.2021.24.6.510
Optimal First-Line Antibiotic Treatment for Pediatric Complicated Appendicitis Based on Peritoneal Fluid Culture
Abstract
Purpose: Consensus is lacking regarding the optimal antibiotic treatment for pediatric complicated appendicitis. This study determined the optimal first-line antibiotic treatment for pediatric patients with complicated appendicitis based on peritoneal fluid cultures.
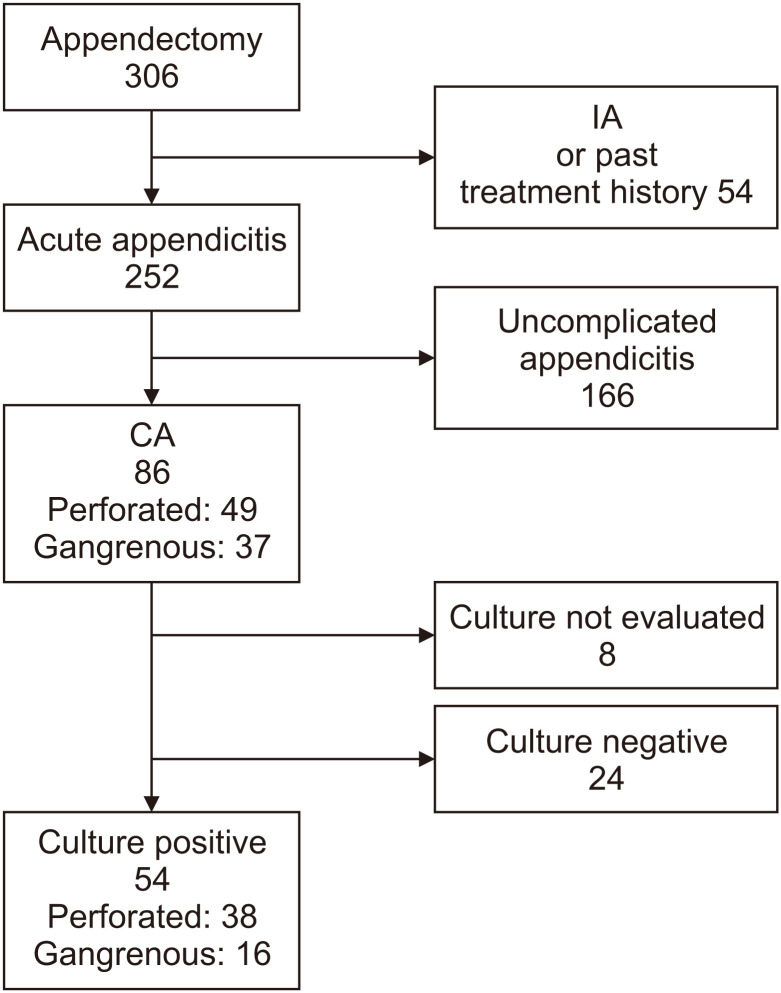
Methods: This retrospective study examined the cases of pediatric patients who underwent appendectomy for complicated appendicitis at our institution between 2013 and 2019. Peritoneal fluid specimens obtained during appendectomy were cultured for the presence of bacteria.
Results: Eighty-six pediatric patients were diagnosed with complicated appendicitis. Of them, bacteria were identified in 54 peritoneal fluid samples. The major identified bacteria were Escherichia coli (n=36 [66.7%]), Bacteroides fragilis (n=28 [51.9%]), α-Streptococcus (n=25 [46.3%]), Pseudomonas aeruginosa (n=10 [18.5%]), Enterococcus avium (n=9 [16.7%]), γ-Streptococcus (n=9 [16.7%]), and Klebsiella oxytoca (n=6 [11.1%]). An antibiotic susceptibility analysis showed E. coli was inhibited by sulbactam/ampicillin in 43.8% of cases versus cefmetazole in 100% of cases. Tazobactam/piperacillin and meropenem inhibited the growth of 96.9-100% of the major identified bacteria. E. coli (100% vs. 84.6%) and P. aeruginosa (100% vs. 80.0%) were more susceptible to amikacin than gentamicin.
Conclusion: Tazobactam/piperacillin or meropenem is a reasonable first-line antibiotic treatment for pediatric complicated appendicitis. In the case of aminoglycoside use, amikacin is recommended.
Keywords: Antibiotics; Complicated appendicitis; Culture; Pediatric; Peritoneal fluid.
Copyright © 2021 by The Korean Society of Pediatric Gastroenterology, Hepatology and Nutrition.
Conflict of interest statement
Conflict of Interest: The authors have no financial conflicts of interest.
Figures
References
-
- Hadley GP. Intra-abdominal sepsis--epidemiology, aetiology and management. Semin Pediatr Surg. 2014;23:357–362. - PubMed
-
- Jimbo T, Masumoto K, Takayasu H, Shinkai T, Urita Y, Uesugi T, et al. Outcome of early discharge protocol after appendectomy for pediatric acute appendicitis. Pediatr Int. 2017;59:803–806. - PubMed
-
- Centers for Disease Control and Prevention (CDC) Surgical site infection (SSI) event: procedure-associated module [Internet] Atlanta (GA): CDC; 2016. [cited 2018 Sep 11]. Available from: https://www.cdc.gov/nhsn/pdfs/pscmanual/9pscssicurrent.pdf.
-
- David IB, Buck JR, Filler RM. Rational use of antibiotics for perforated appendicitis in childhood. J Pediatr Surg. 1982;17:494–500. - PubMed
-
- Elmore JR, Dibbins AW, Curci MR. The treatment of complicated appendicitis in children. What is the gold standard? Arch Surg. 1987;122:424–427. - PubMed