

Magnetic Sphincter Augmentation Outcomes in Severe Gastroesophageal Reflux Disease
- PMID: 34796181
- PMCID: PMC8592890
- DOI: 10.3389/fmed.2021.645592
Magnetic Sphincter Augmentation Outcomes in Severe Gastroesophageal Reflux Disease
Abstract
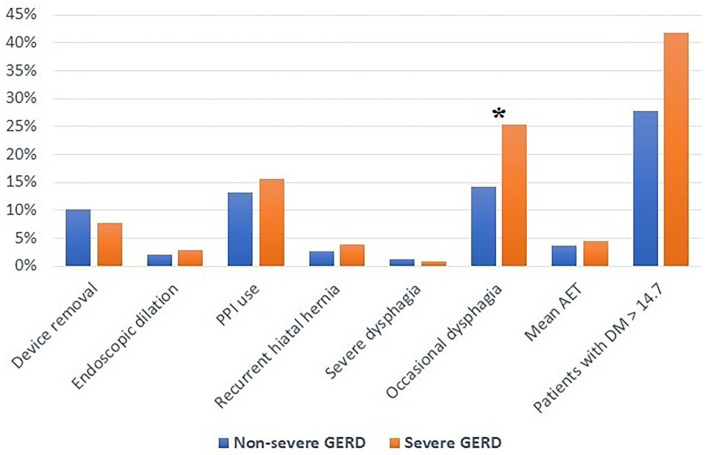
Introduction: Outcomes of laparoscopic procedures for gastroesophageal reflux disease (GERD) are variable depending on surgical expertise and/or patient-related factors. Some procedures may be inadequate in patients with severe disease. Effectiveness of laparoscopic magnetic sphincter augmentation (MSA) has not been extensively tested in patients with severe disease. Methods: A prospectively collected database was analyzed to identify patients who underwent MSA at a single institution. Individuals who had previous esophago-gastric surgery were excluded. Severe GERD was defined as lower esophageal sphincter pressure <5 mmHg, distal esophageal amplitude <30 mmHg, Barrett's metaplasia, stricture or grade C-D esophagitis, and/or DeMeester score >50. Clinical characteristics and outcomes of patients with severe GERD were compared with those of patients with mild to moderate GERD who served as control group. Results: Over the study period, a total of 336 patients met the inclusion criteria, and 102 (30.4%) had severe GERD. The median follow-up was 24 months (IQR = 75) in severe GERD patients and 32 months (IQR = 84) in those with non-severe GERD. Patients with severe GERD had a higher rate of dysphagia and higher GERD-HRQL scores. After the MSA procedure, symptoms, health-related quality of life scores, and proton-pump inhibitors consumption significantly decreased in both groups (p < 0.05). No difference between groups was found in the prevalence of severe post-operative dysphagia, the need for endoscopic dilation or device removal, and the DeMeester score. Conclusion: Laparoscopic MSA is safe and effective in reducing symptoms, PPI use, and esophageal acid exposure also in patients with severe GERD.
Keywords: Barrett's esophagus; DeMeester score; esophagitis; gastroesophageal reflux disease; hiatus hernia; magnetic sphincter augmentation.
Copyright © 2021 Ferrari, Siboni, Riva, Guerrazzi, Lovece and Bonavina.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures




References
LinkOut - more resources
Full Text Sources
Miscellaneous