

Diets for weight management in adults with type 2 diabetes: an umbrella review of published meta-analyses and systematic review of trials of diets for diabetes remission
- PMID: 34796367
- PMCID: PMC8660762
- DOI: 10.1007/s00125-021-05577-2
Diets for weight management in adults with type 2 diabetes: an umbrella review of published meta-analyses and systematic review of trials of diets for diabetes remission
Abstract
Aims/hypothesis: Weight reduction is fundamental for type 2 diabetes management and remission, but uncertainty exists over which diet type is best to achieve and maintain weight loss. We evaluated dietary approaches for weight loss, and remission, in people with type 2 diabetes to inform practice and clinical guidelines.
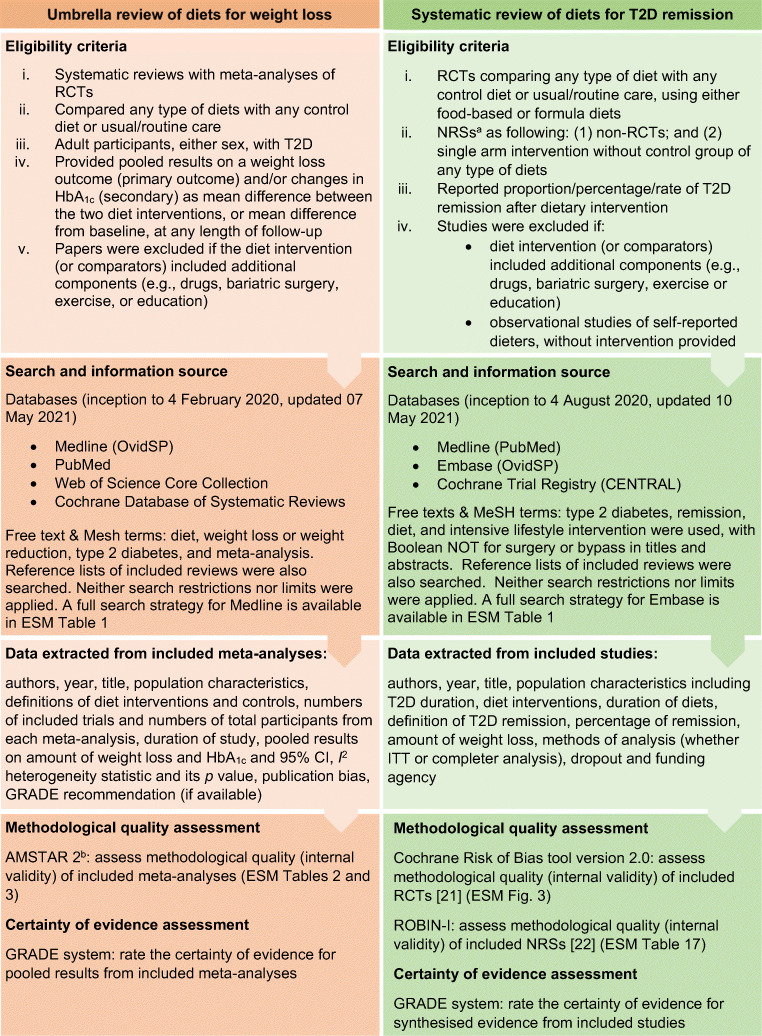
Methods: First, we conducted a systematic review of published meta-analyses of RCTs of weight-loss diets. We searched MEDLINE (Ovid), PubMed, Web of Science and Cochrane Database of Systematic Reviews, up to 7 May 2021. We synthesised weight loss findings stratified by diet types and assessed meta-analyses quality with A Measurement Tool to Assess Systematic Reviews (AMSTAR) 2. We assessed certainty of pooled results of each meta-analysis using Grading of Recommendations, Assessment, Development and Evaluations (GRADE) (PROSPERO CRD42020169258). Second, we conducted a systematic review of any intervention studies reporting type 2 diabetes remission with weight-loss diets, in MEDLINE (via PubMed), Embase and Cochrane Central Register of Controlled Trials, up to 10 May 2021. Findings were synthesised by diet type and study quality (Cochrane Risk of Bias tool 2.0 and Risk Of Bias In Non-randomised Studies - of Interventions [ROBINS-I]), with GRADE applied (PROSPERO CRD42020208878).
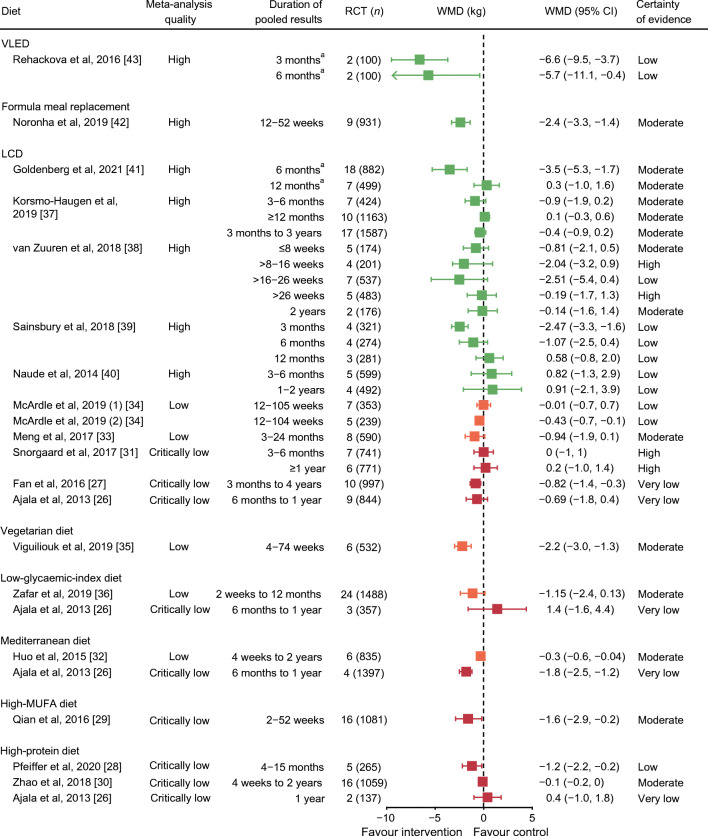
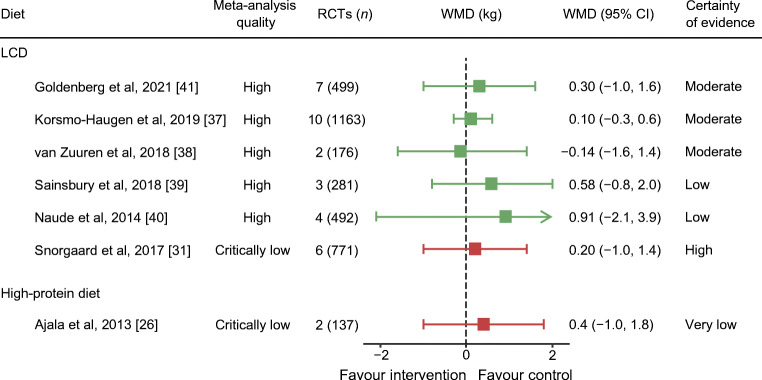
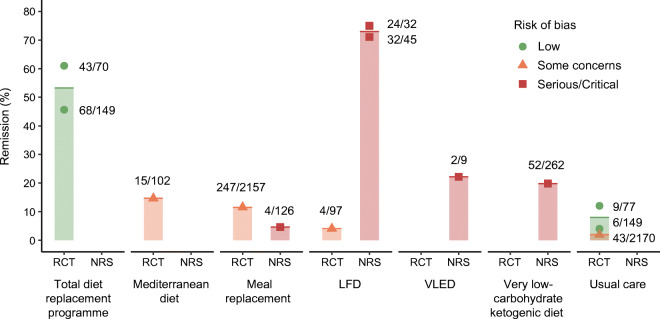
Results: We identified 19 meta-analyses of weight-loss diets, involving 2-23 primary trials (n = 100-1587), published 2013-2021. Twelve were 'critically low' or 'low' AMSTAR 2 quality, with seven 'high' quality. Greatest weight loss was reported with very low energy diets, 1.7-2.1 MJ/day (400-500 kcal) for 8-12 weeks (high-quality meta-analysis, GRADE low), achieving 6.6 kg (95% CI -9.5, -3.7) greater weight loss than low-energy diets (4.2-6.3 MJ/day [1000-1500 kcal]). Formula meal replacements (high quality, GRADE moderate) achieved 2.4 kg (95% CI -3.3, -1.4) greater weight loss over 12-52 weeks. Low-carbohydrate diets were no better for weight loss than higher-carbohydrate/low-fat diets (high quality, GRADE high). High-protein, Mediterranean, high-monounsaturated-fatty-acid, vegetarian and low-glycaemic-index diets all achieved minimal (0.3-2 kg) or no difference from control diets (low to critically low quality, GRADE very low/moderate). For type 2 diabetes remission, of 373 records, 16 met inclusion criteria. Remissions at 1 year were reported for a median 54% of participants in RCTs including initial low-energy total diet replacement (low-risk-of-bias study, GRADE high), and 11% and 15% for meal replacements and Mediterranean diets, respectively (some concerns for risk of bias in studies, GRADE moderate/low). For ketogenic/very low-carbohydrate and very low-energy food-based diets, the evidence for remission (20% and 22%, respectively) has serious and critical risk of bias, and GRADE certainty is very low.
Conclusions/interpretation: Published meta-analyses of hypocaloric diets for weight management in people with type 2 diabetes do not support any particular macronutrient profile or style over others. Very low energy diets and formula meal replacement appear the most effective approaches, generally providing less energy than self-administered food-based diets. Programmes including a hypocaloric formula 'total diet replacement' induction phase were most effective for type 2 diabetes remission. Most of the evidence is restricted to 1 year or less. Well-conducted research is needed to assess longer-term impacts on weight, glycaemic control, clinical outcomes and diabetes complications.
Keywords: Diet; Evidence-based guidelines; Informed clinical practice; Meta-analysis; Quality assessment; Randomised trial; Remission; Systematic review; Type 2 diabetes; Weight loss.
© 2021. The Author(s).
Figures
References
-
- International Diabetes Federation (2017) IDF Diabetes Atlas. Available from www.diabetesatlas.org. Accessed 10 Oct 2019
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
