

Assessment of Pretreatment With Oral P2Y12 Inhibitors and Cardiovascular and Bleeding Outcomes in Patients With Non-ST Elevation Acute Coronary Syndromes: A Systematic Review and Meta-analysis
- PMID: 34797371
- PMCID: PMC8605486
- DOI: 10.1001/jamanetworkopen.2021.34322
Assessment of Pretreatment With Oral P2Y12 Inhibitors and Cardiovascular and Bleeding Outcomes in Patients With Non-ST Elevation Acute Coronary Syndromes: A Systematic Review and Meta-analysis
Abstract
Importance: The practice of pretreatment with oral P2Y12 inhibitors in non-ST elevation acute coronary syndromes (NSTEACS) remains common; however, its association with improved cardiovascular outcomes is unclear.
Objective: To assess the association between oral P2Y12 inhibitor pretreatment and cardiovascular and bleeding outcomes in patients with NSTEACS.
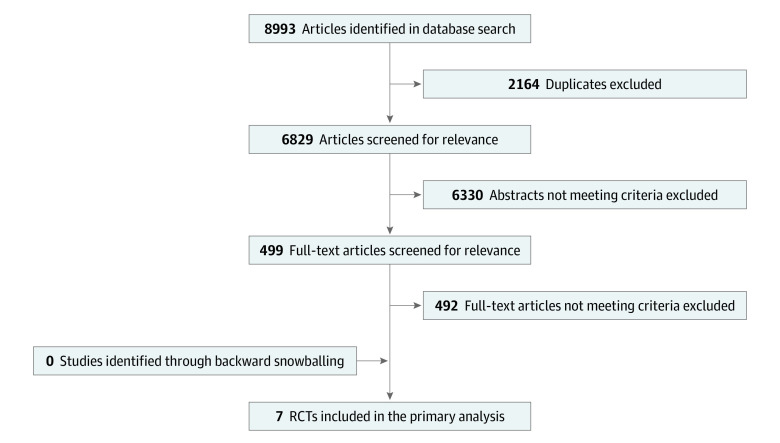
Data sources: On March 20, 2021, PubMed, MEDLINE, Embase, Scopus, Web of Science, Science Direct, clinicaltrials.gov, and the Cochrane Central Register for Controlled Trials were searched from database inception.
Study selection: Randomized clinical trials of patients with NSTEACS randomized to either oral P2Y12 inhibitor pretreatment (defined as prior to angiography) or no pretreatment (defined as following angiography, once coronary anatomy was known) among patients undergoing an invasive strategy.
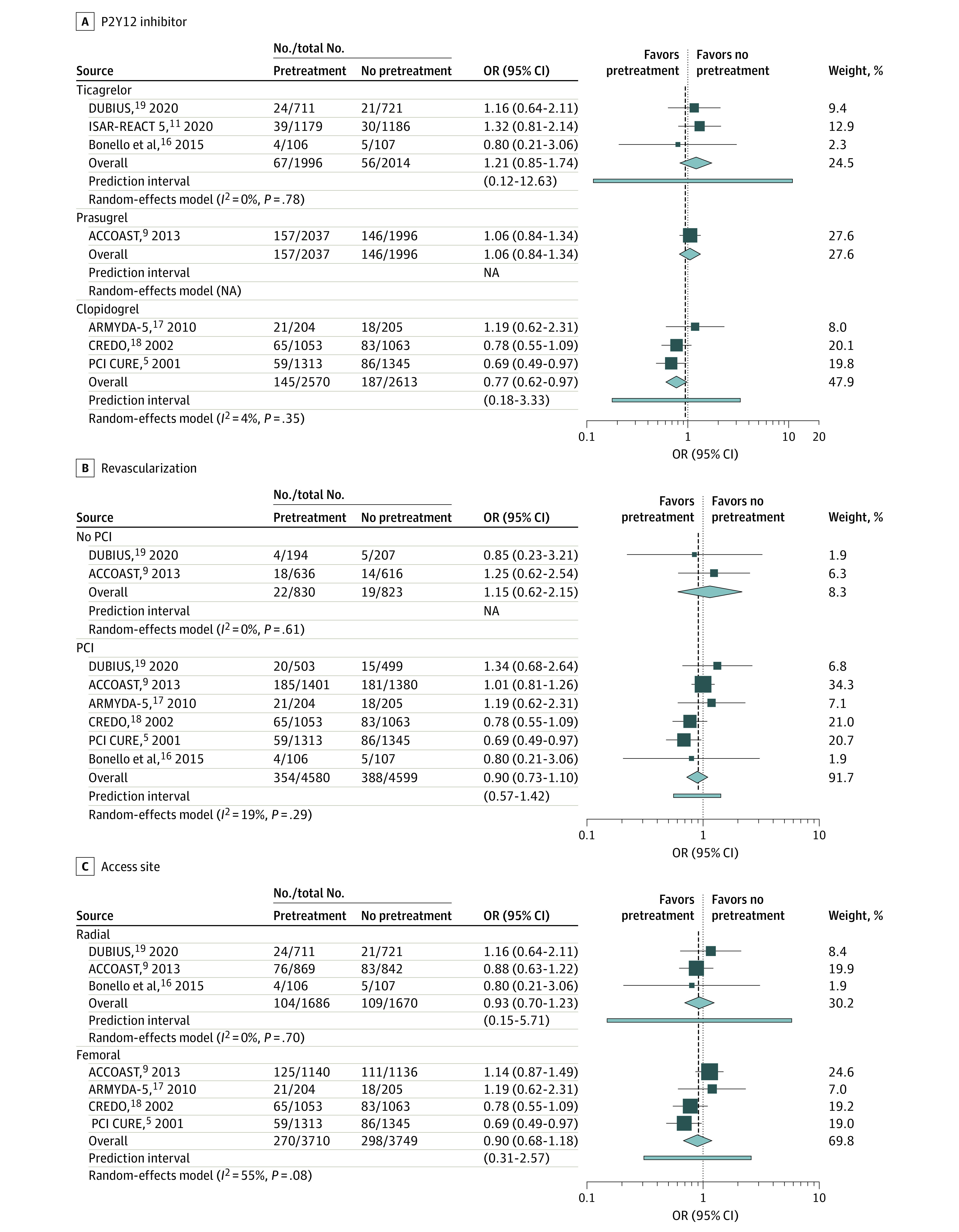
Data extraction and synthesis: This study followed Preferred Reporting Items for Systematic Reviews and Meta-analyses guidelines. Data on publication year, sample size, clinical characteristics, revascularization strategy, P2Y12 inhibitor type and dosage, time from pretreatment to angiography, and end point data were independently extracted by 2 authors. A random-effects model was used, including stratification by (1) P2Y12 inhibitor type, (2) revascularization strategy, and (3) access site.
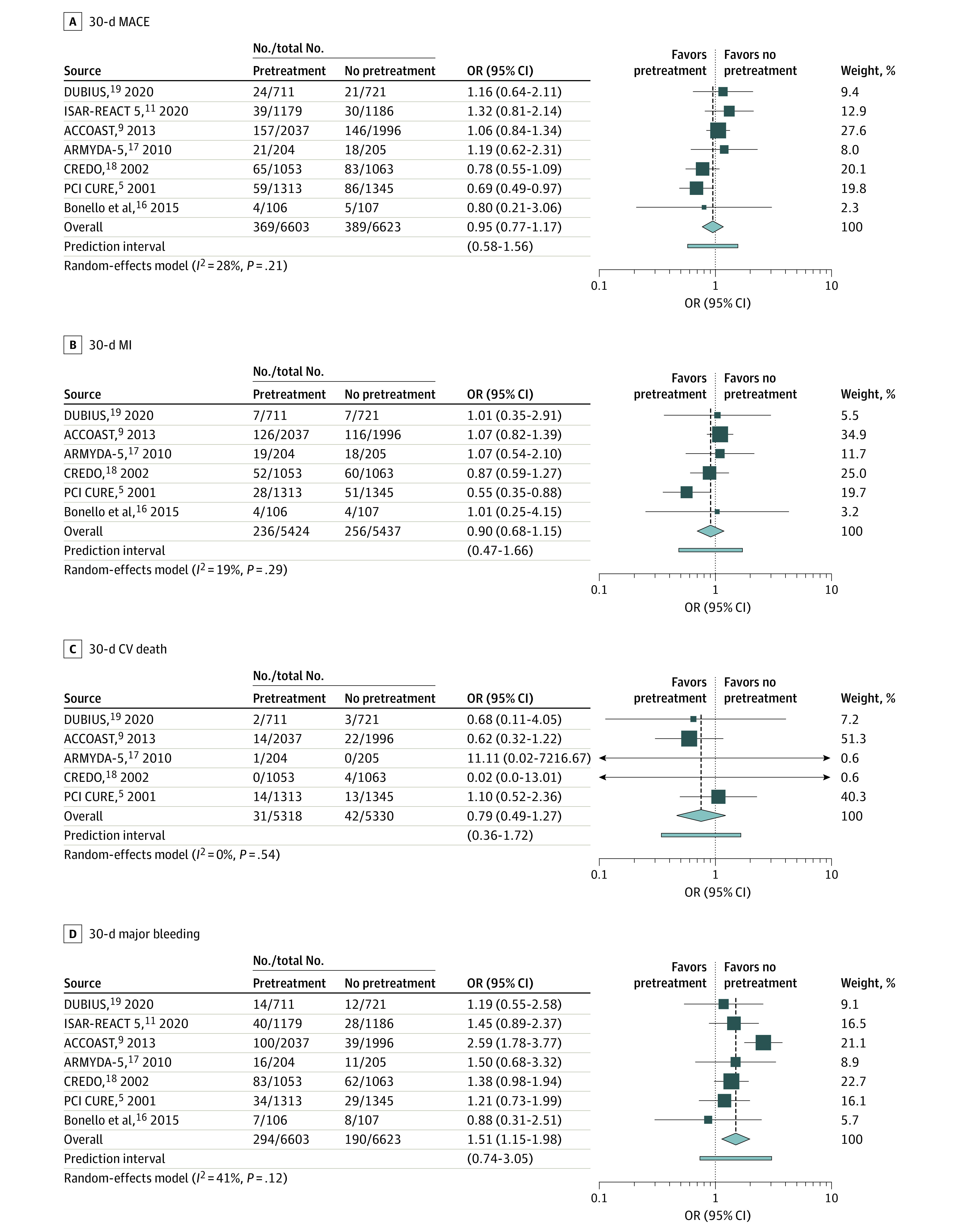
Main outcomes and measures: The primary end point was 30-day major adverse cardiac events (MACEs). Secondary end points were 30-day myocardial infarction (MI) and cardiovascular death. The primary safety end point was 30-day major bleeding (defined according to individual studies).
Results: A total of 7 trials randomizing 13 226 patients to either pretreatment (6603 patients) or no pretreatment (6623 patients) were included. The mean age of patients was 64 years and 3598 (27.2%) were female individuals. Indication for P2Y12 inhibitors was non-ST elevation myocardial infarction in 7430 patients (61.7%), radial access was used in 4295 (32.6%), and 10 945 (82.8%) underwent percutaneous coronary intervention. Pretreatment was not associated with a reduction in 30-day MACE (odds ratio [OR], 0.95; 95% CI, 0.78-1.15; I2 = 28%), 30-day MI (OR, 0.90; 95% CI, 0.72-1.12; I2 = 19%), or 30-day cardiovascular death (OR, 0.79; 95% CI, 0.49-1.27; I2 = 0%). The risk of 30-day major bleeding was increased among patients who underwent pretreatment (OR, 1.51; 95% CI, 1.16-1.97; I2 = 41%). The number needed to harm to bring about 1 major bleeding event with oral P2Y12 inhibitor pretreatment was 63 patients.
Conclusions and relevance: In this study, pretreatment with oral P2Y12 inhibitors among patients with NSTEACS prior to angiography, compared with treatment once coronary anatomy is known, was associated with increased bleeding risk and no difference in cardiovascular outcomes. Routine pretreatment with oral P2Y12 inhibitors in patients with NSTEACS receiving an early invasive strategy is not supported by this study.
Conflict of interest statement
Figures
Comment in
-
Pretreatment in the Setting of Non-ST-Elevated Acute Coronary Syndrome-When It Is Time to Change.JAMA Netw Open. 2021 Nov 1;4(11):e2134472. doi: 10.1001/jamanetworkopen.2021.34472. JAMA Netw Open. 2021. PMID: 34797373 No abstract available.
References
-
- Mehta SR, Yusuf S, Peters RJ, et al. ; Clopidogrel in Unstable angina to prevent Recurrent Events trial (CURE) Investigators . Effects of pretreatment with clopidogrel and aspirin followed by long-term therapy in patients undergoing percutaneous coronary intervention: the PCI-CURE study. Lancet. 2001;358(9281):527-533. doi:10.1016/S0140-6736(01)05701-4 - DOI - PubMed
