

Anti-Drug Antibody Formation Against Biologic Agents in Inflammatory Bowel Disease: A Systematic Review and Meta-Analysis
- PMID: 34797516
- PMCID: PMC9826743
- DOI: 10.1007/s40259-021-00507-5
Anti-Drug Antibody Formation Against Biologic Agents in Inflammatory Bowel Disease: A Systematic Review and Meta-Analysis
Abstract
Background and aims: Immunogenicity with formation of anti-drug antibodies (ADA) to biologics is an important reason for treatment failure in inflammatory bowel disease (IBD). Our aim was to assess the rate of ADA, the effect of combination therapy with immunomodulators on ADA and the influence of ADA on efficacy and safety of biologics for IBD treatment.
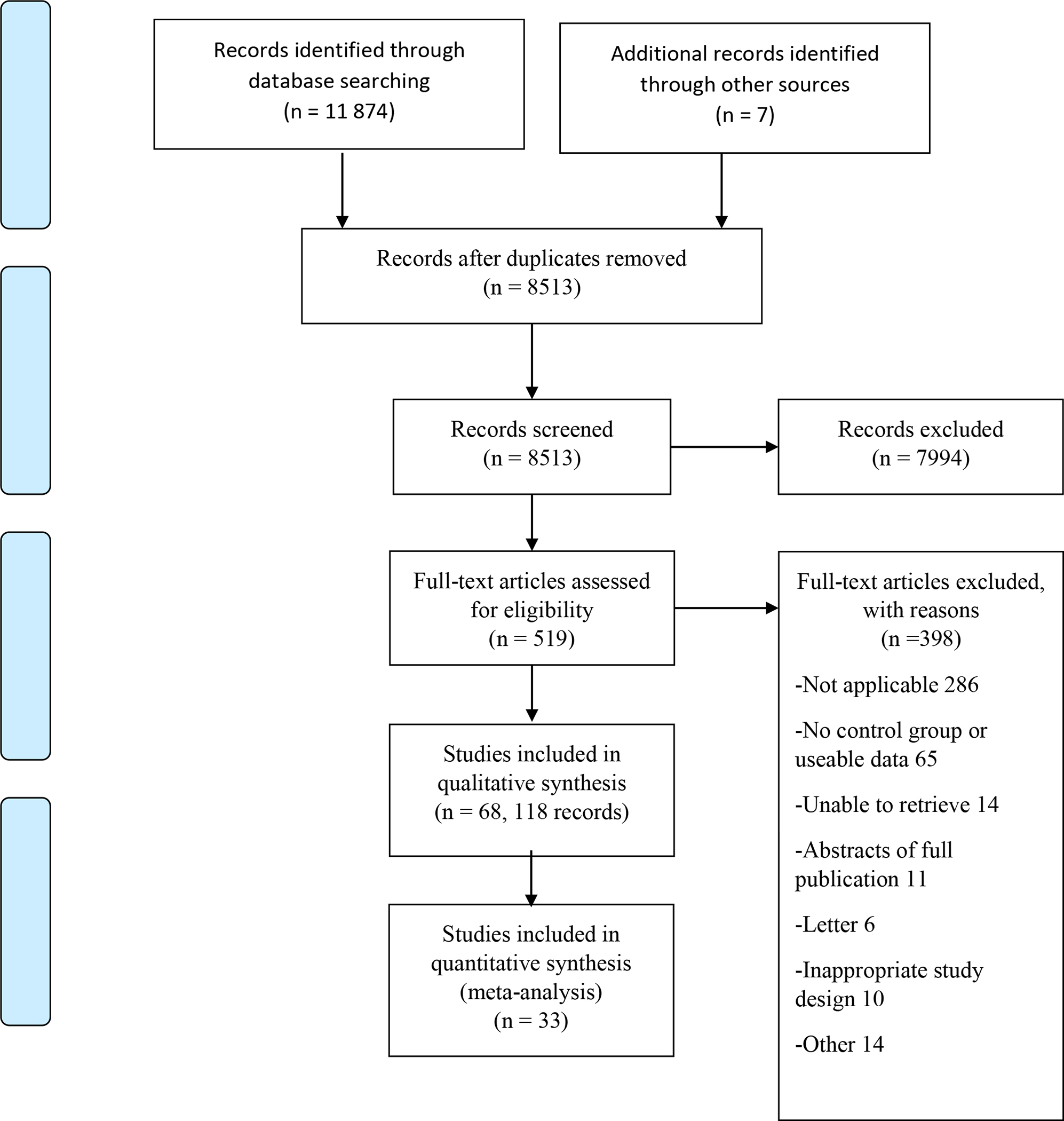
Methods: MEDLINE, Embase and Cochrane Central Register of Controlled Trials (CENTRAL) were searched from inception to April 2020 for trials of biologics that assessed immunogenicity. The overall certainty of evidence was evaluated using Grading of Recommendations, Assessment, Development and Evaluations (GRADE). The primary outcome was rate of ADA. Secondary outcomes included efficacy and safety outcomes among patients with detectable versus undetectable ADA. For dichotomous outcomes, pooled risk ratios (RR) and 95% confidence intervals (CI) were calculated.
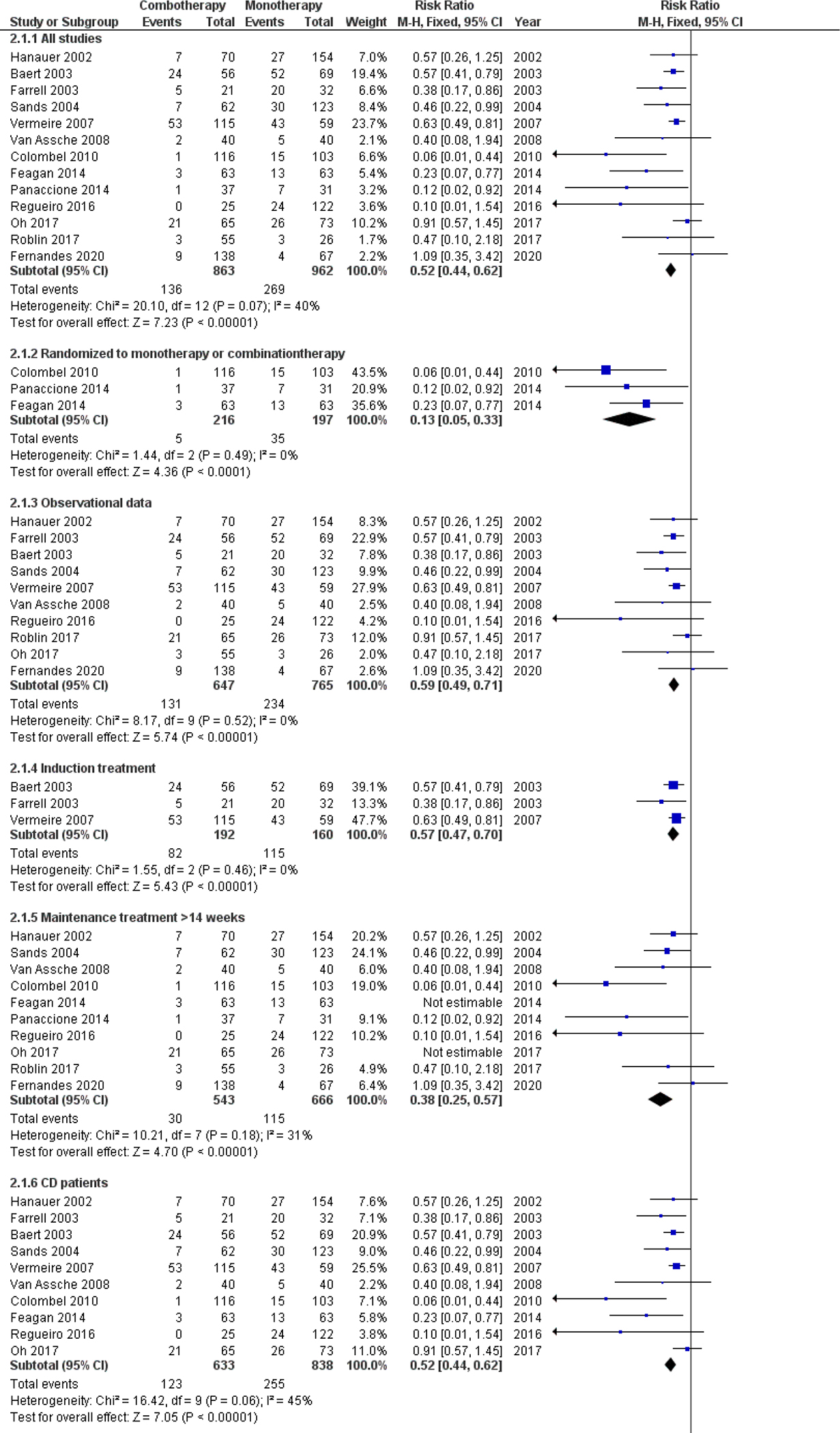
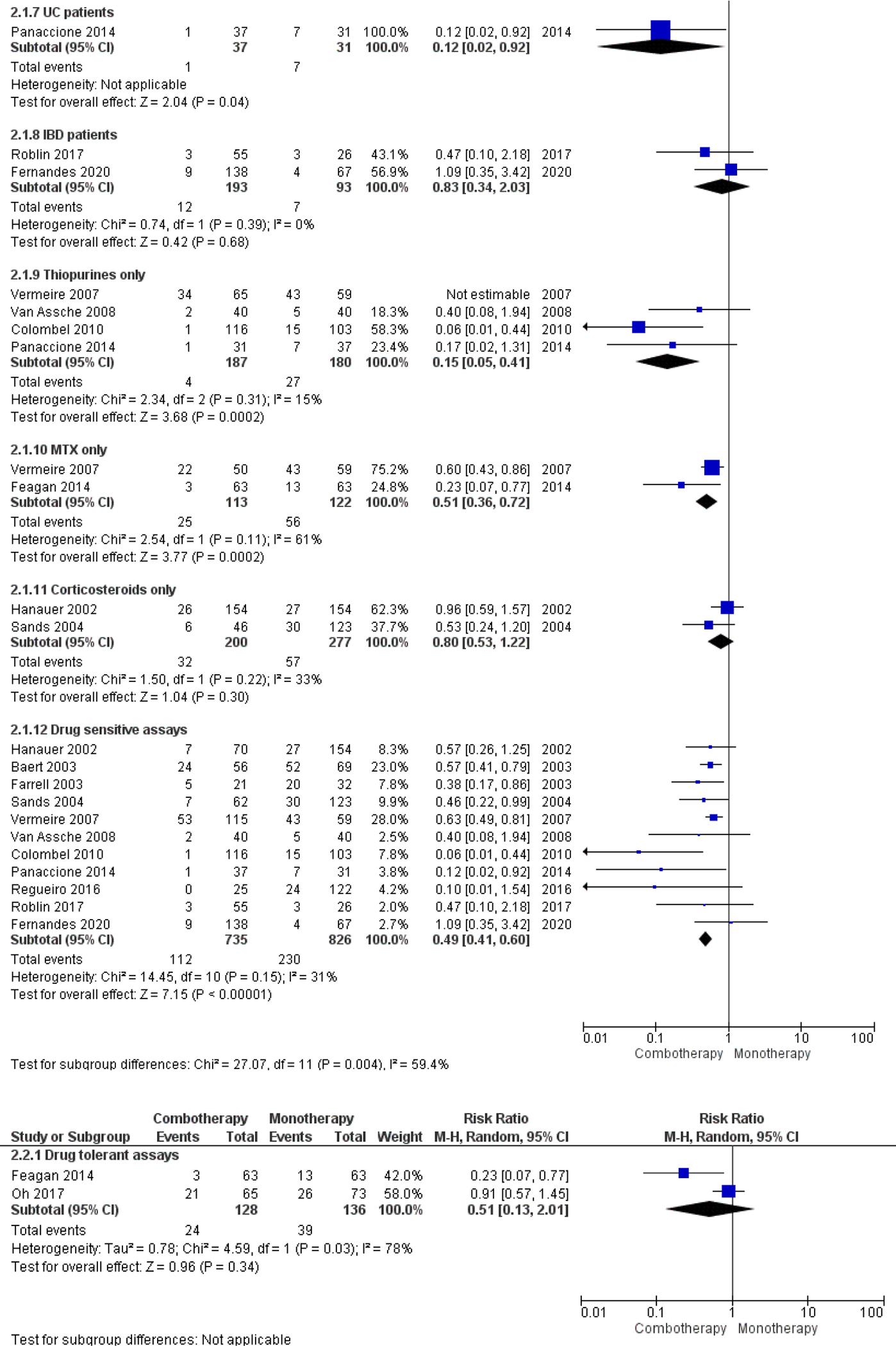
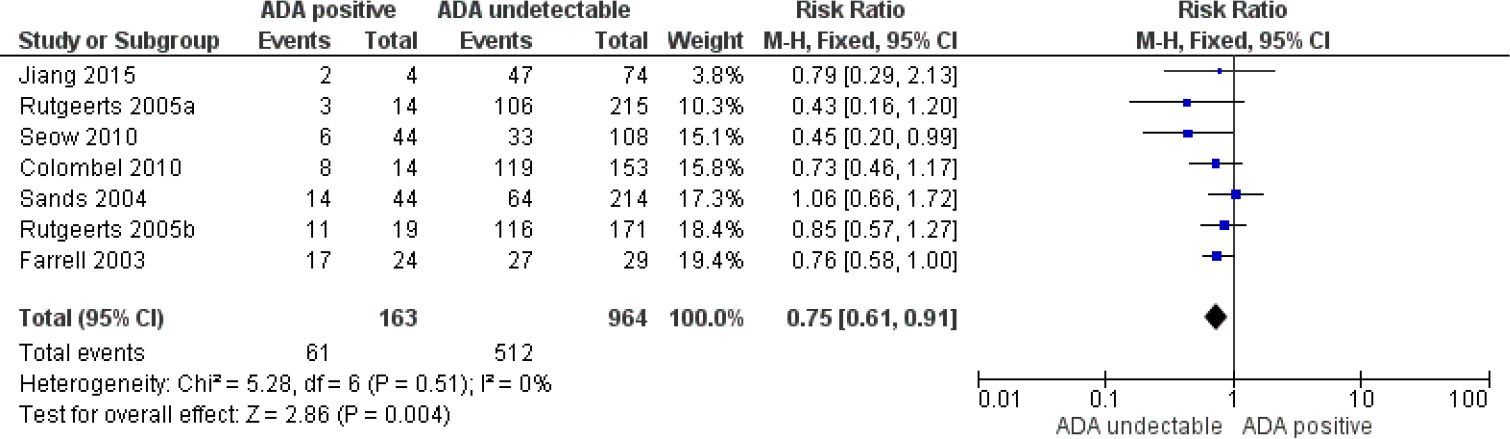
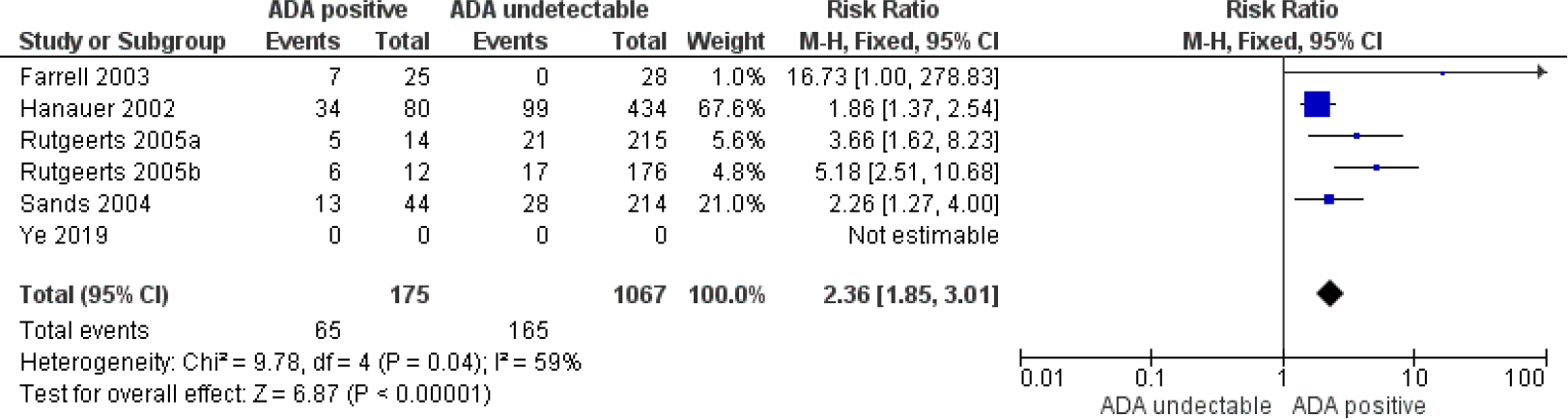
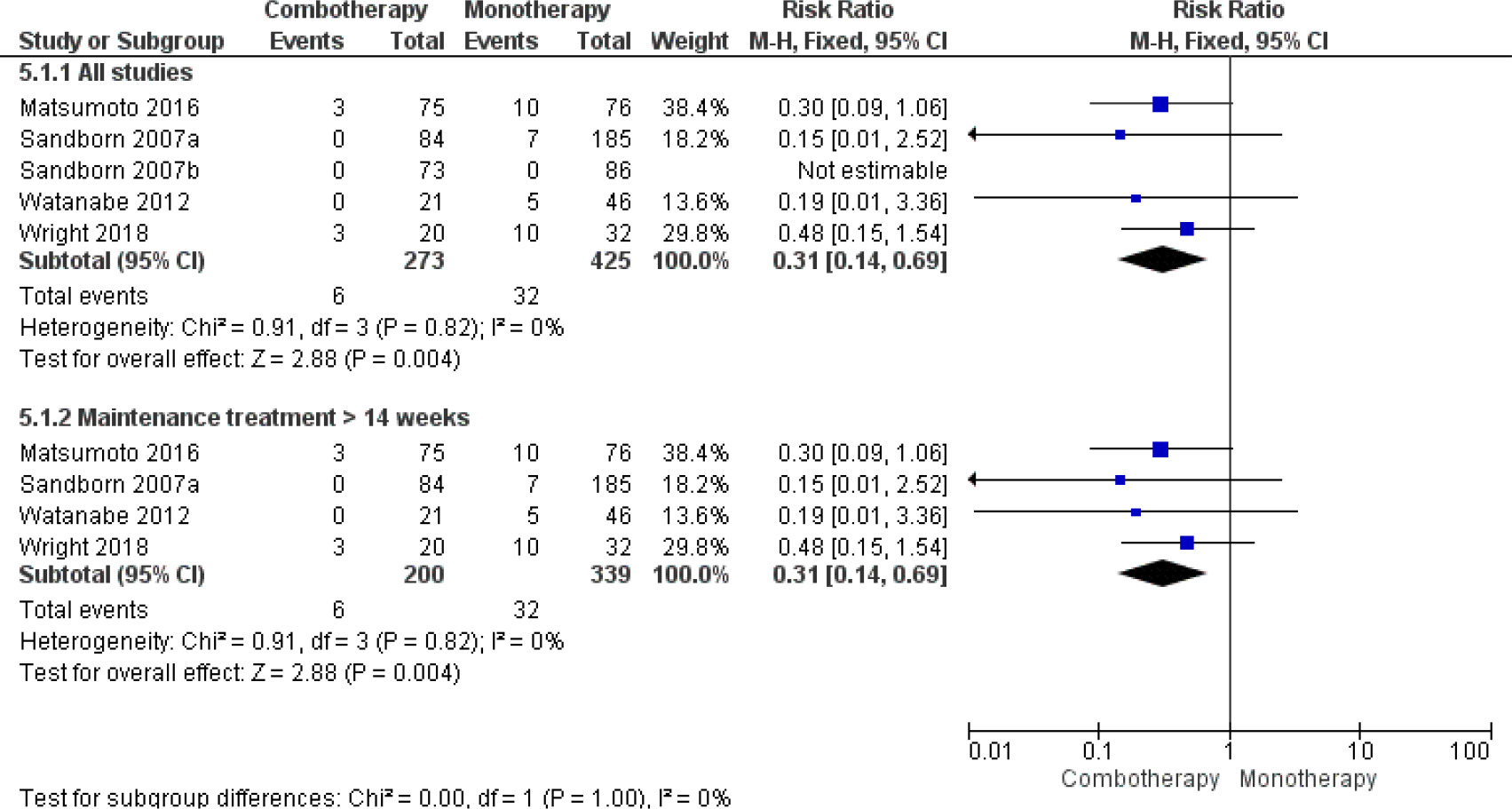
Results: Data from 68 studies were analyzed and 33 studies (5850 patients) were included in the meta-analysis. Pooled ADA rates for biologic monotherapy were 28.0% for infliximab, 7.5% for adalimumab, 3.8% for golimumab, 10.9% for certolizumab, 6.2% for ustekinumab and 16.0% for natalizumab. Pooled ADA rates were 8.4% for vedolizumab and 5.0% for etrolizumab for combo- and monotherapy combined. In all biologics, ADA rates were underestimated by use of drug-sensitive ADA assays and higher dose and/or frequency. ADA rate was significantly reduced in patients treated with combination therapy for infliximab (RR 0.52; 95% CI 0.44-0.62), adalimumab (RR 0.31; 95% CI 0.14-0.69), golimumab (RR 0.29; 95% CI 0.10-0.83), certolizumab pegol (RR 0.30; 95% CI 0.14-0.67) and natalizumab (RR 0.20; 95% CI 0.11-0. 39). ADA to infliximab were associated with lower clinical response rates (RR 0.75; 95% CI 0.61-0.91) and higher rates of infusion reactions (RR 2.36; 95% CI 1.85-3.01).
Conclusions: Differences in analytical methods to detect ADA hamper comparison of true ADA rates across biologics in IBD. Use of combination therapy with immunomodulators appeared to reduce ADA positivity for most biologics. For infliximab, ADA were associated with reduced drug efficacy and increased adverse events.
© 2021. The Author(s), under exclusive licence to Springer Nature Switzerland AG.
Figures

References
-
- van der Valk ME, Mangen MJ, Leenders M, Dijkstra G, van Bodegraven AA, Fidder HH, et al. Healthcare costs of inflammatory bowel disease have shifted from hospitalisation and surgery towards anti-TNFalpha therapy: results from the COIN study. Gut. 2014;63(1):72–9. - PubMed
-
- Bots SJA, Hoekman DR, Benninga MA, Ponsioen CY, D’Haens GR, Lowenberg M. Patterns of anti-TNF use and associated treatment outcomes in inflammatory bowel disease patients: results from an analysis of Dutch health insurance claims data. The Netherlands journal of medicine. 2017;75(10):432–42. - PubMed
-
- Plevy SE, Landers CJ, Prehn J, Carramanzana NM, Deem RL, Shealy D, et al. A role for TNF-alpha and mucosal T helper-1 cytokines in the pathogenesis of Crohn’s disease. Journal of immunology (Baltimore, Md : 1950). 1997;159(12):6276–82. - PubMed
-
- Masuda H, Iwai S, Tanaka T, Hayakawa S. Expression of IL-8, TNF-alpha and IFN-gamma m-RNA in ulcerative colitis, particularly in patients with inactive phase. Journal of clinical & laboratory immunology. 1995;46(3):111–23. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
