

Phase 3, randomized, open-label study of pembrolizumab plus lenvatinib versus chemotherapy for first-line treatment of advanced or recurrent endometrial cancer: ENGOT-en9/LEAP-001
- PMID: 34799418
- PMCID: PMC8762038
- DOI: 10.1136/ijgc-2021-003017
Phase 3, randomized, open-label study of pembrolizumab plus lenvatinib versus chemotherapy for first-line treatment of advanced or recurrent endometrial cancer: ENGOT-en9/LEAP-001
Abstract
Background: Pembrolizumab plus lenvatinib is a novel combination with promising efficacy in patients with advanced and recurrent endometrial cancer. This combination demonstrated high objective response rates in a single-arm phase 1b/2 trial of lenvatinib plus pembrolizumab in patients with advanced endometrial cancer (KEYNOTE-146/Study 111) after ≤2 previous lines of therapy. In a randomized phase 3 trial of lenvatinib in combination with pembrolizumab versus treatment of physician's choice in patients with advanced endometrial cancer (KEYNOTE-775/Study 309), after 1‒2 previous lines of therapy (including neoadjuvant/adjuvant), this combination improved objective response rates, progression-free survival, and overall survival compared with chemotherapy.
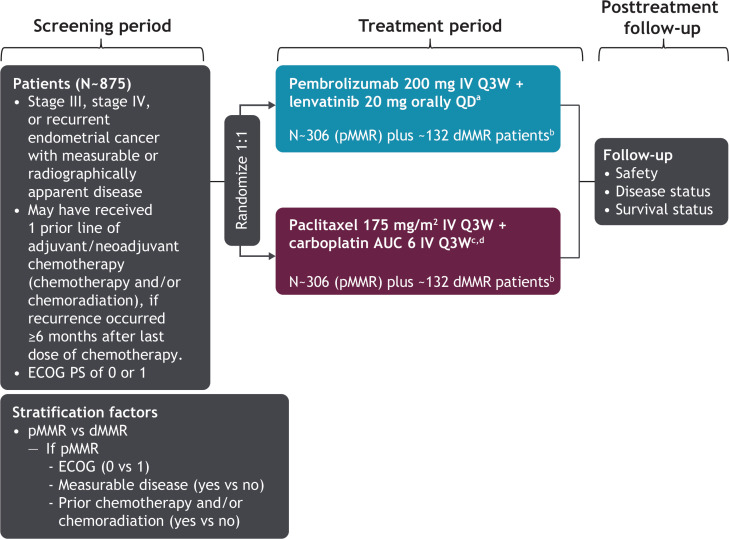
Primary objective: To compare the efficacy and safety of first-line pembrolizumab plus lenvatinib versus paclitaxel plus carboplatin in patients with newly diagnosed stage III/IV or recurrent endometrial cancer, with measurable or radiographically apparent disease.
Study hypothesis: Pembrolizumab plus lenvatinib is superior to chemotherapy with respect to progression-free survival and overall survival in patients with mismatch repair-proficient tumors and all patients (all-comers).
Trial design: Phase 3, randomized (1:1), open-label, active-controlled trial. Patients will receive pembrolizumab intravenously every 3 weeks plus lenvatinib orally daily or paclitaxel plus carboplatin intravenously every 3 weeks, stratified by mismatch repair status (proficient vs deficient). Patients with mismatch repair-proficient tumors will be further stratified by Eastern Cooperative Oncology Group performance status (0/1), measurable disease (yes/no), and prior chemotherapy and/or chemoradiation (yes/no).
Major inclusion/exclusion criteria: Adults with stage III/IV/recurrent histologically confirmed endometrial cancer that is measurable or radiographically apparent per blinded independent central review. Patients may have received previous chemotherapy only as neoadjuvant/adjuvant therapy and/or concurrently with radiation. Patients with carcinosarcoma (malignant mixed Müllerian tumor), endometrial leiomyosarcoma, or other high grade sarcomas, or endometrial stromal sarcomas were excluded.
Primary endpoints: Progression-free and overall survival (dual primary endpoints).
Sample size: About 875 patients.
Estimated dates for completing accrual and presenting results: Enrollment is expected to take approximately 24 months, with presentation of results in 2022.
Trial registration: ClinicalTrials.gov, NCT03884101.
Keywords: endometrial neoplasms; uterine cancer.
© IGCS and ESGO 2022. Re-use permitted under CC BY. Published by BMJ.
Conflict of interest statement
Competing interests: CM: funded research, EU, FWF, AstraZeneca, and Roche; honoraria/expenses, Roche, Novartis, Amgen, Merck, Pharmamar, AstraZeneca, Tesaro, and GSK; consulting/advisory board, Roche, Novartis, Amgen, Merck, AstraZeneca, Pfizer, Pharmamar, Cerulean, Vertex, GSK, Seagen, and Eisai. AT: funded research, AstraZeneca, Roche, MSD, and RUSSCO; honoraria/expenses, AstraZeneca, Roche, MSD, Eisai, Biocad, and RUSSCO; consulting/advisory board, AstraZeneca, Pfizer, MSD, Eisai, Tesaro, and Biocad. SP: honoraria, MSD, Eisai, GSK, AstraZeneca, Clovis, Pfizer, Pharmamar, and Roche. LG: institutional grants from AstraZeneca, Pfizer, Merck Sharp & Dohme, Karyopharm, Tesaro, IMV, Alkermes, Clovis, ImmunoGen Inc, Roche, Mersana, Esperas, Novocure GmbH, and OncoQuest Pharmaceuticals; advisory boards, AstraZeneca, GSK, Eisai, Eisai-Merck, and Alkermes. DK: clinical trials, Roche, Lilly Oncology, Clovis, MSD, Abbvie, Takeda, Novartis, Pfizer, Array BioPharma Inc, Servier, Nektar Therapeutics, Merck Healthcare KGaA, and GlaxoSmithKline; consultancy, Roche, Boehringer Ingelheim, Pfizer, MSD, BMS, Novartis, AstraZeneca, Raffo-tecnofarma, Varifarma, and Bayer. MJR: consulting/advisory board, MSD, AstraZeneca, GSK, Pharmamar, and Roche. SF: consulting/advisory board, Akesobio; honoraria/expenses, Amgen. MM-M: consulting/advisory board, Roche, Eli-Lilly, BMS, AstraZeneca, Teva, Amgen, Bayer, and Pfizer. RB: travel expenses, Clovis Oncology, Roche, and MSD. CV: study funding for present publication from MSD; institutional grant, MSD; consulting fees, Janssen-Cilag, Roche, GSK, Atheneum Partners, Astellas Pharma, MSD, BMS, and Leo-Pharma; payment or honoraria for presentations, Janssen Cilag, Leo Pharma, and Bayer; payment or honoraria for advisory boards, Janssen Cilag, Leo Pharma, MSD, GSK, and AstraZeneca; support for travel, Roche and Pfizer. KH: funded research, MSD, Ono, Takeda, Daiichi-Sankyo, and Eisai; honoraria, Takeda, Chugai, Kyowa-Kirin, Genmab, AstraZeneca, and MSD; consulting/advisory board, MSD, Eisai, and Takeda. EB: funded research, EU, DLR, AstraZeneca, Roche Diagnostics, and Bayer; honoraria/expenses, Roche, Merck, AstraZeneca, Tesaro, GSK, Clovis, Roche Diagnostics, Molecular Health, and Eisai; consulting/advisory board, Roche, Eisai, Merck, AstraZeneca, GSK, and Clovis. JM: employee of Eisai Inc, Woodcliff Lake, New Jersey, USA. JJL: employee of Merck Sharp & Dohme Corp, a subsidiary of Merck & Co Inc, Kenilworth, New Jersey, USA and stockholder in Merck & Co. VM: study support (all funding to institution)/consultant/advisory board membership, Merck, Eisai, Karyopharm, AstraZeneca, Clovis, Moreo, Takeda, Zymeworks, and Genentech; supported in part by the NIH/NCI Cancer Center Support grant P30 CA008748.
Figures
References
-
- Howlader N, Noone AM, Krapcho M, et al., eds. SEER Cancer Statistics Review, 1975-2017. Bethesda, MD: National Cancer Institute, 2020. https://seer.cancer.gov/csr/1975_2017/
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
