

Glial Fibrillary Acidic Protein Autoimmunity: A French Cohort Study
- PMID: 34799461
- PMCID: PMC8829963
- DOI: 10.1212/WNL.0000000000013087
Glial Fibrillary Acidic Protein Autoimmunity: A French Cohort Study
Abstract
Background and objectives: To report the clinical, biological, and imaging features and clinical course of a French cohort of patients with glial fibrillary acidic protein (GFAP) autoantibodies.
Methods: We retrospectively included all patients who tested positive for GFAP antibodies in the CSF by immunohistochemistry and confirmed by cell-based assay using cells expressing human GFAPα since 2017 from 2 French referral centers.
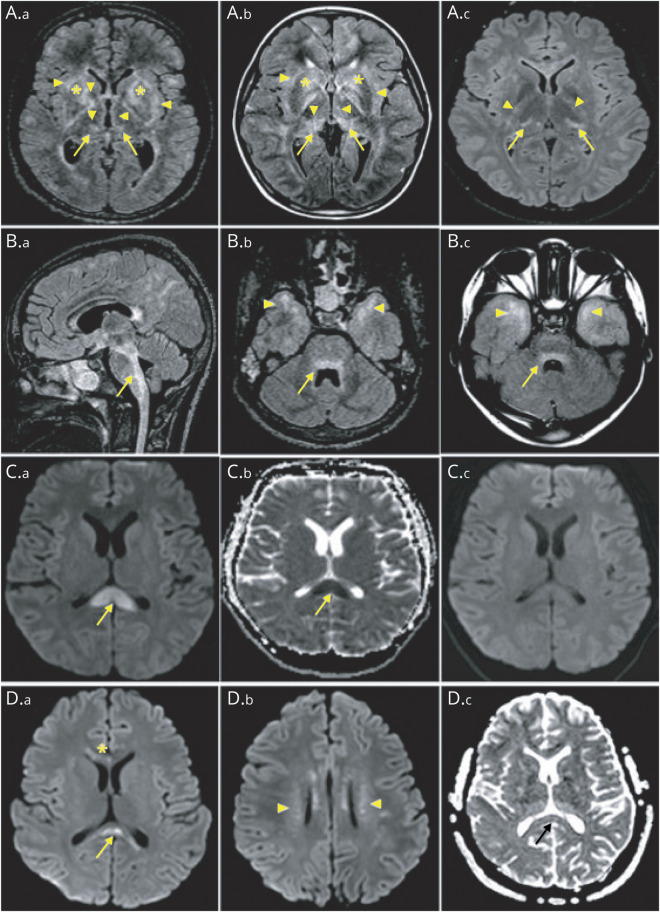
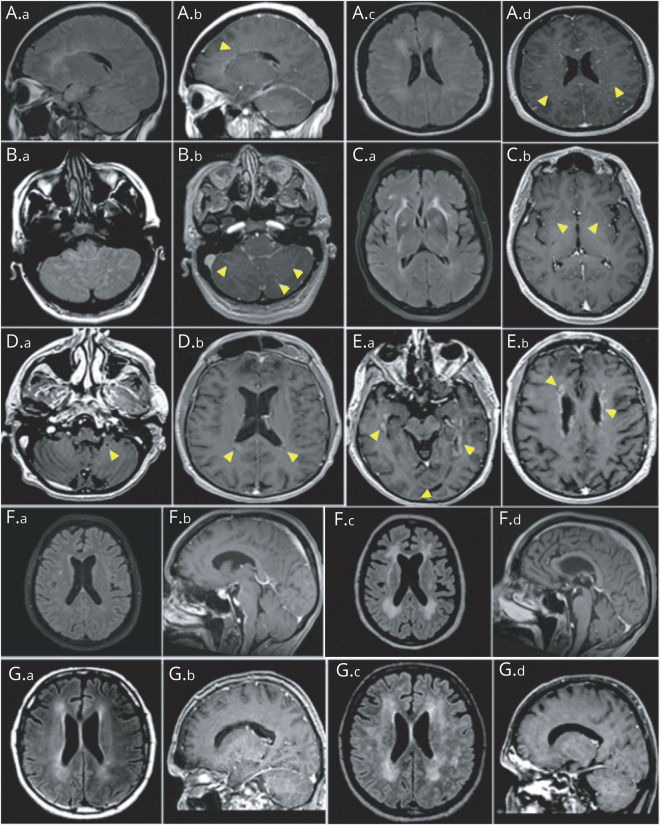
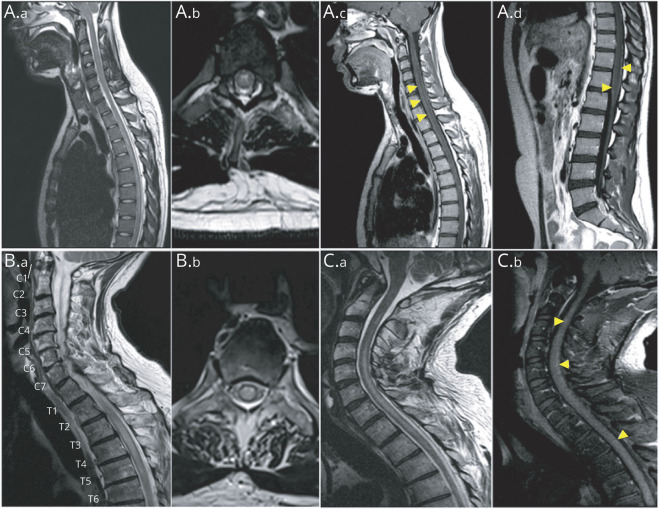
Results: We identified 46 patients with GFAP antibodies. Median age at onset was 43 years, and 65% were men. Infectious prodromal symptoms were found in 82%. Other autoimmune diseases were found in 22% of patients, and coexisting neural autoantibodies in 11%. Tumors were present in 24%, and T-cell dysfunction in 23%. The most frequent presentation was subacute meningoencephalitis (85%), with cerebellar dysfunction in 57% of cases. Other clinical presentations included myelitis (30%) and visual (35%) and peripheral nervous system involvement (24%). MRI showed perivascular radial enhancement in 32%, periventricular T2 hyperintensity in 41%, brainstem involvement in 31%, leptomeningeal enhancement in 26%, and reversible splenial lesions in 4 cases. A total of 33 of 40 patients had a monophasic course, associated with a good outcome at last follow-up (Rankin Score ≤2: 89%), despite a severe clinical presentation. Adult and pediatric features are similar. Thirty-two patients were treated with immunotherapy. A total of 11/22 patients showed negative conversion of GFAP antibodies.
Discussion: GFAP autoimmunity is mainly associated with acute/subacute meningoencephalomyelitis with prodromal symptoms, for which tumors and T-cell dysfunction are frequent triggers. The majority of patients followed a monophasic course with a good outcome.
Copyright © 2022 The Author(s). Published by Wolters Kluwer Health, Inc. on behalf of the American Academy of Neurology.
Figures
Comment in
-
Glial Fibrillary Acidic Protein Immunoglobulin G in CSF: A Biomarker of Severe but Reversible Encephalitis.Neurology. 2022 Feb 8;98(6):221-222. doi: 10.1212/WNL.0000000000013089. Epub 2021 Nov 19. Neurology. 2022. PMID: 34799465 No abstract available.
References
-
- Fang B, McKeon A, Hinson SR. Autoimmune glial fibrillary acidic protein astrocytopathy: a novel meningoencephalomyelitis. JAMA Neurol. 2016;73(11):1297-1307. - PubMed
-
- Flanagan EP, Hinson SR, Lennon VA. Glial fibrillary acidic protein immunoglobulin G as biomarker of autoimmune astrocytopathy: analysis of 102 patients. Ann Neurol. 2017;81(2):298-309. - PubMed
-
- Dubey D, Hinson SR, Jolliffe EA. Autoimmune GFAP astrocytopathy: prospective evaluation of 90 patients in 1 year. J Neuroimmunol. 2018;321:157-163. - PubMed
-
- Long Y, Liang J, Xu H. Autoimmune glial fibrillary acidic protein astrocytopathy in Chinese patients: a retrospective study. Eur J Neurol. 2018;25(3):477-483. - PubMed
-
- Yang X, Liang J, Huang Q. Treatment of autoimmune glial fibrillary acidic protein astrocytopathy: follow-up in 7 cases. Neuroimmunomodulation. 2017;24(2):113-119. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous