

Peri-interventional outcome study in the elderly in Europe: A 30-day prospective cohort study
- PMID: 34799496
- PMCID: PMC8815832
- DOI: 10.1097/EJA.0000000000001639
Peri-interventional outcome study in the elderly in Europe: A 30-day prospective cohort study
Abstract
Objectives: The aim of this study was to describe the 30-day mortality rate of patients aged 80 years and older undergoing surgical and nonsurgical procedures under anaesthesia in Europe and to identify risk factors associated with mortality.
Design: A prospective cohort study.
Setting: European multicentre study, performed from October 2017 to December 2018. Centres committed to a 30-day recruitment period within the study period.
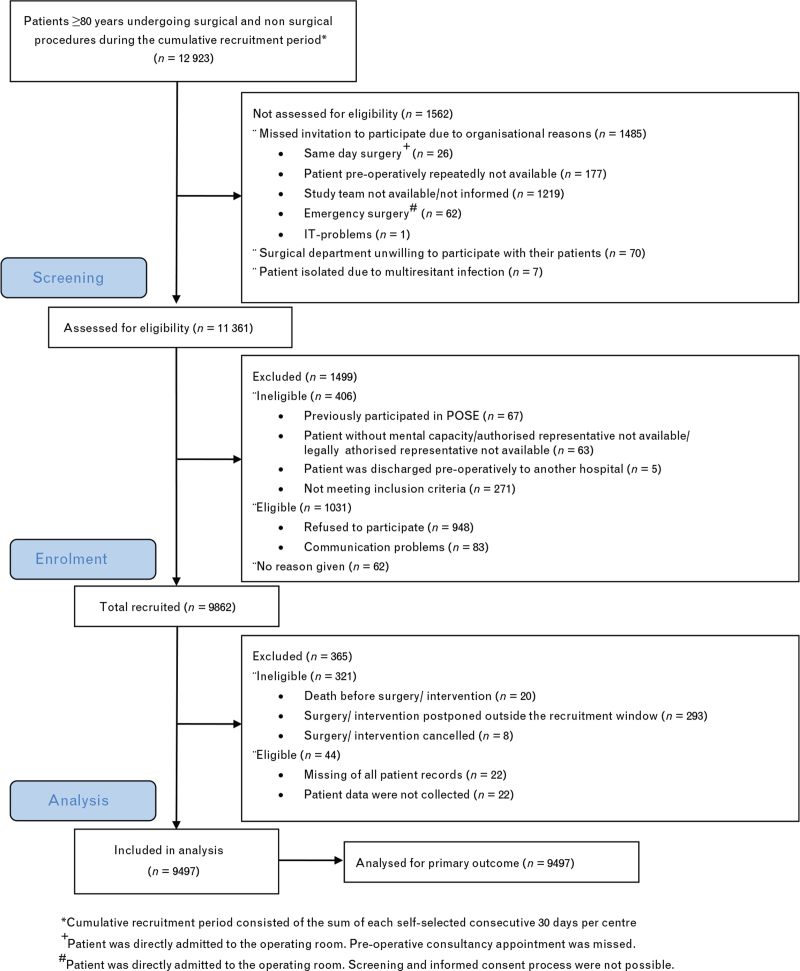
Patients: Nine thousand four hundred and ninety-seven consecutively recruited patients aged 80 years and older undergoing any kind of surgical or nonsurgical procedures under anaesthesia.
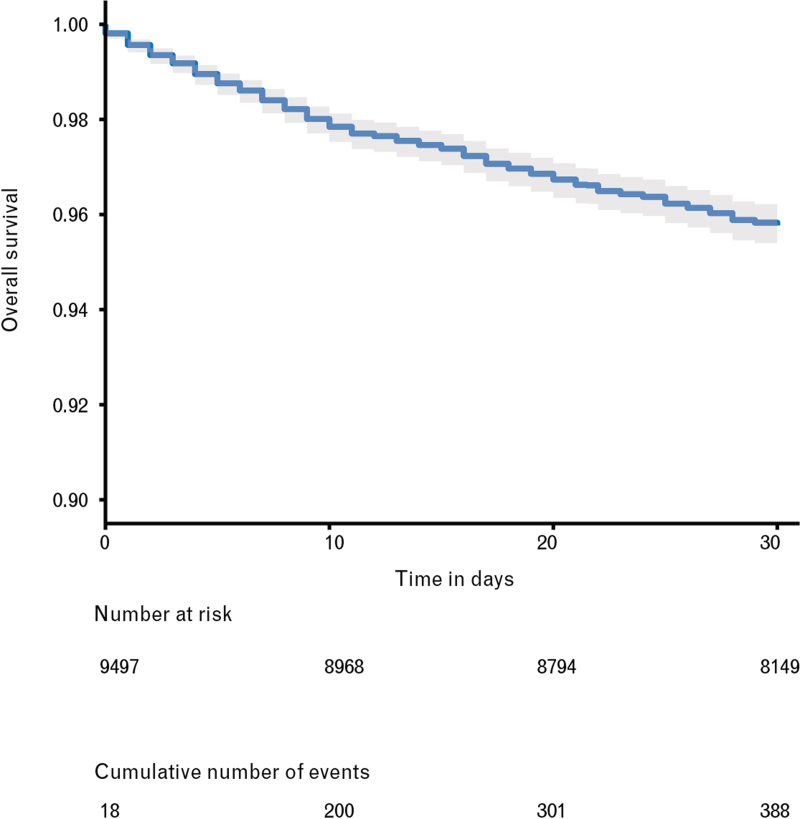
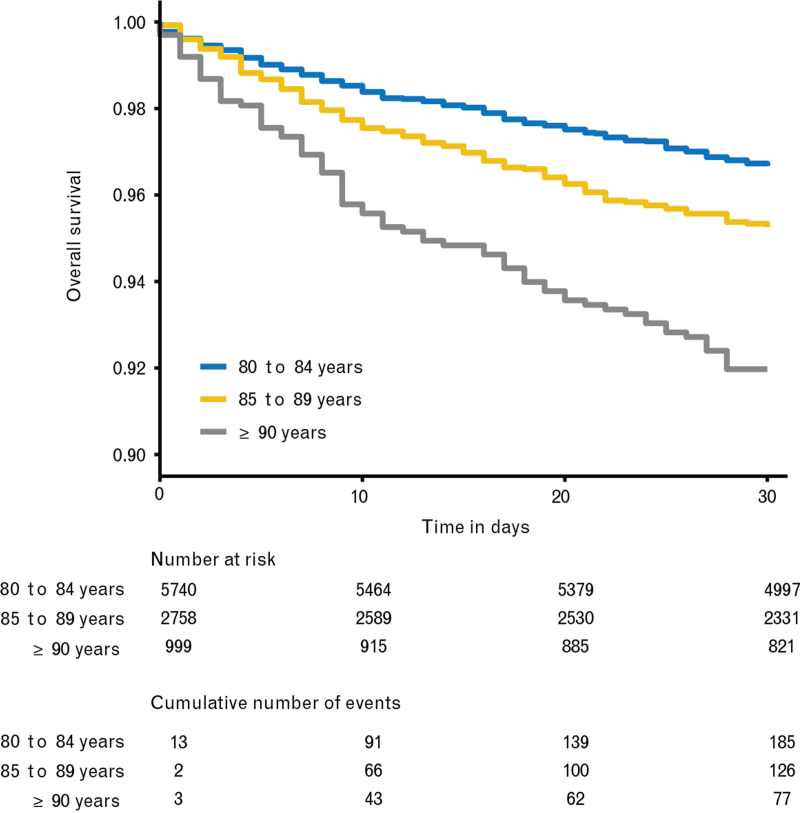
Main outcome measures: The primary outcome was all-cause mortality within 30 days after procedure described by Kaplan-Meier curves with 95% CI. Risk factors for 30-day mortality were analysed using a Cox regression model with 14 fixed effects and a random centre effect.
Results: Data for 9497 patients (median age, 83.0 years; 52.8% women) from 177 academic and nonacademic hospitals in 20 countries were analysed. Patients presented with multimorbidity (77%), frailty (14%) and at least partial functional dependence (38%). The estimated 30-day mortality rate was 4.2% (95% CI 3.8 to 4.7). Among others, independent risk factors for 30-day mortality were multimorbidity, hazard ratio 1.87 (95% CI 1.26 to 2.78), frailty, hazard ratio 2.63 (95% CI 2.10 to 3.30), and limited mobility, hazard ratio 2.19 (95% CI 1.24 to 3.86). The majority of deaths (76%) occurred in hospital. Mortality risk for unplanned ICU admission was higher, hazard ratio 3.57 (95% CI 2.38 to 5.26) than for planned ICU admission, hazard ratio 1.92 (95% CI 1.47 to 2.50). Compared with other studies, the in-hospital complication rates of 17.4 and 3.9% after discharge were low. Admission to a unit with geriatric care within 30 days after the intervention was associated with a better survival within the first 10 days.
Conclusions: The estimated 30-day mortality rate of 4.2% was lower than expected in this vulnerable population.
Trial registration: ClinicalTrials.gov Identifier: NCT03152734, https://clinicaltrials.gov.
Copyright © 2021 The Author(s). Published by Wolters Kluwer Health, Inc. on behalf of the European Society of Anaesthesiology and Intensive Care.
Figures
Comment in
-
Strike a pose: The POSE study poses some questions!Eur J Anaesthesiol. 2022 Mar 1;39(3):193-195. doi: 10.1097/EJA.0000000000001658. Eur J Anaesthesiol. 2022. PMID: 35115452 No abstract available.
References
-
- WHO. Global strategy and action plan on ageing and health. 2017. https://www.who.int/ageing/WHO-GSAP-2017.pdf?ua=1 [Accessed 20 April 2021].
-
- WHO. Aging and health. https://www.who.int/en/news-room/fact-sheets/detail/ageing-and-health [Accessed 20 April 2021].
-
- Hoogendijk EO, Afilalo J, Ensrud KE, et al. Frailty: implications for clinical practice and public health. Lancet 2019; 394:1365–1375. - PubMed
-
- Dent E, Martin FC, Bergman H, et al. Management of frailty: opportunities, challenges, and future directions. Lancet 2019; 394:1376–1386. - PubMed
-
- WHO. World report on aging and health. 2015. https://apps.who.int/iris/bitstream/handle/10665/186463/9789240694811_en... [Accessed 02 May 2021].
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
