

Duodenal Microbiome and Serum Metabolites Predict Hepatocellular Carcinoma in a Multicenter Cohort of Patients with Cirrhosis
- PMID: 34799768
- PMCID: PMC9287237
- DOI: 10.1007/s10620-021-07299-2
Duodenal Microbiome and Serum Metabolites Predict Hepatocellular Carcinoma in a Multicenter Cohort of Patients with Cirrhosis
Abstract
Background: Hepatocellular carcinoma (HCC) is rapidly increasing in the U.S. and is a leading cause of mortality for patients with cirrhosis. Discovering novel biomarkers for risk stratification of HCC is paramount. We examined biomarkers of the gut-liver axis in a prospective multicenter cohort.
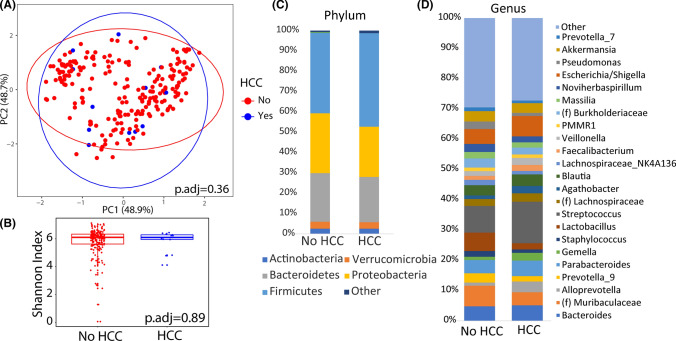
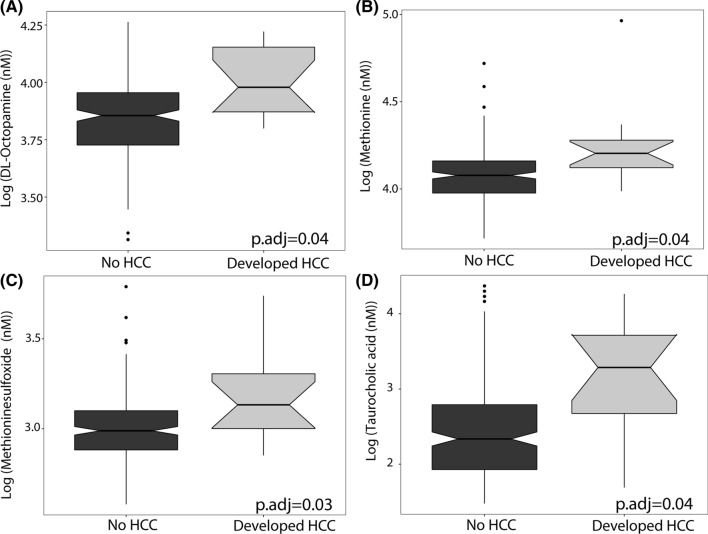
Methods: Patients with cirrhosis without a history of HCC were recruited between May 2015 and March 2020 and prospectively followed at 3 tertiary care hospitals in Los Angeles. Microbiome analysis was performed on duodenal biopsies and metabolomic analysis was performed on serum samples, collected at the time of enrollment. Optimal microbiome-based survival analysis and Cox proportional hazards regression analysis were used to determine microbiota and metabolite associations with HCC development, respectively.
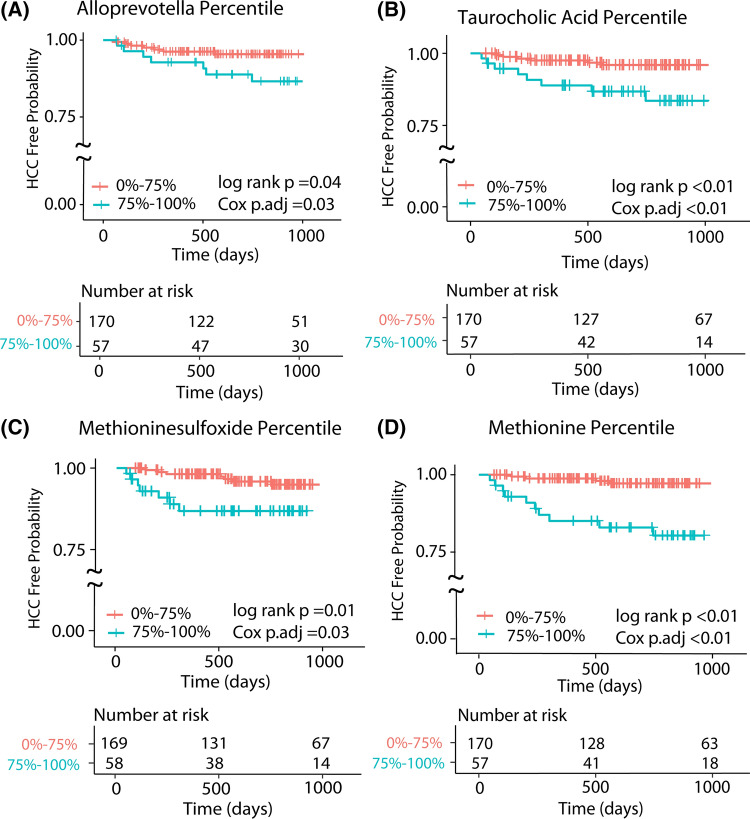
Results: A total of 227 participants with liver cirrhosis contributed a total of 459.58 person-years of follow-up, with 14 incident HCC diagnoses. Male sex (HR = 7.06, 95% CI = 1.02-54.86) and baseline hepatic encephalopathy (HE, HR = 4.65, 95% CI = 1.60-13.52) were associated with developing HCC over follow-up. Adjusting for age, sex, baseline HE, and alkaline phosphatase, an increased risk of HCC were observed for participants with the highest versus lowest three quartiles for duodenal Alloprevotella (HR = 3.22, 95% CI = 1.06-9.73) and serum taurocholic acid (HR = 6.87, 95% CI = 2.32-20.27), methionine (HR = 9.97, 95% CI = 3.02-32.94), and methioninesulfoxide (HR = 5.60, 95% CI = 1.84-17.10). Being in the highest quartile for Alloprevotella or methionine had a sensitivity and specificity for developing HCC of 85.71% and 60.56%, respectively, with an odds ratio of 10.92 (95% CI = 2.23-53.48).
Conclusion: Alloprevotella and methionine, methioninesulfoxide, and taurocholic acid predicted future HCC development in a high-risk population of participants with liver cirrhosis.
Keywords: Alloprevotella; Bile acids; Biogenic amines; Methionine; Small intestine; Taurocholic acid; Time-to-event.
© 2021. The Author(s).
Conflict of interest statement
All authors do not have any potential conflicts of interest.
Figures
References
-
- Howlader N, Noone A, Krapcho M, et al. SEER Cancer Statistics Review, 1975–2014. National Cancer Institute. 2018:posted to the SEER web site, April 2017.
